Department of Obstetrics and Gynecology, Erasmus MC, University Medical Center, Dr. Molewaterplein 40, 3015 GD, Rotterdam, The Netherlands.
Department of Biostatistics, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
Reprod Biol Endocrinol. 2021 Nov 4;19(1):164. doi: 10.1186/s12958-021-00843-9.
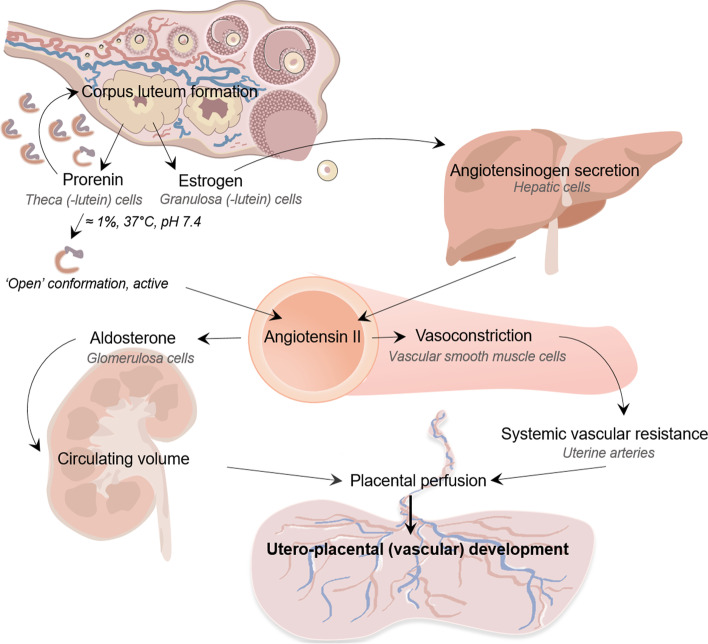
Pregnancies with > 1 corpus luteum (CL) display a hyperdynamic circulation and an increased risk of small-for-gestational age deliveries. Among the factors released by the CL is prorenin, the inactive precursor of renin. Since the renin-angiotensin-aldosterone system (RAAS) is involved in early hemodynamic pregnancy adaptation, we linked both CL number and first-trimester concentrations of prorenin (as an indicator of RAAS activity) and the aldosterone/renin ratio (as an indicator of angiotensin-independent aldosterone effectiveness) to non-invasive markers of utero-placental (vascular) development, measured longitudinally from the first trimester onwards.
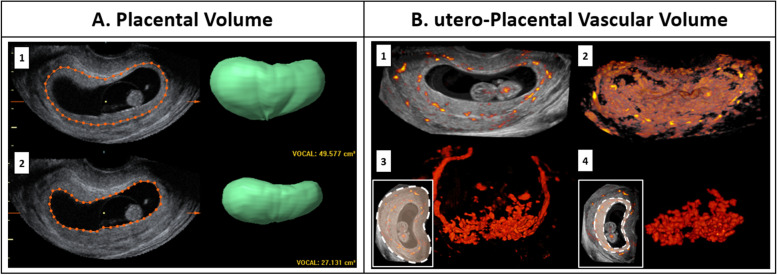
A total of 201 women, who conceived naturally or after in-vitro fertilization treatment (with 0 (n = 8), 1 (n = 143), or > 1 (n = 51) CL), were selected from the Rotterdam Periconceptional Cohort. Maternal RAAS components were determined at 11 weeks gestation. Placental volume and utero-placental vascular volume were measured from transvaginal 3D ultrasound scans at 7, 9 and 11 weeks gestation, pulsatility and resistance indices of the uterine arteries were assessed by pulsed wave Doppler ultrasounds at 7, 9, 11, 13, 22 and 32 weeks gestation. At birth placental weight was obtained using standardized procedures.
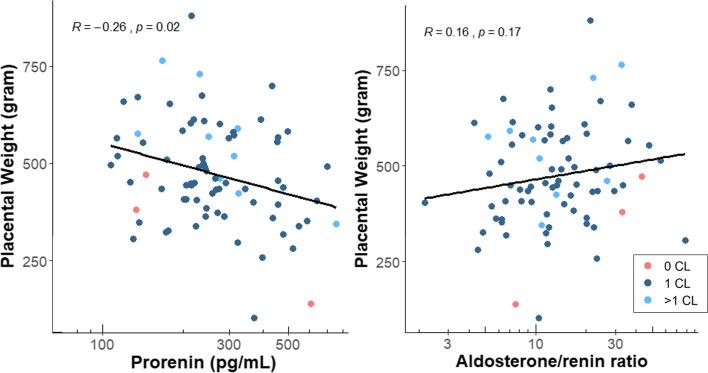
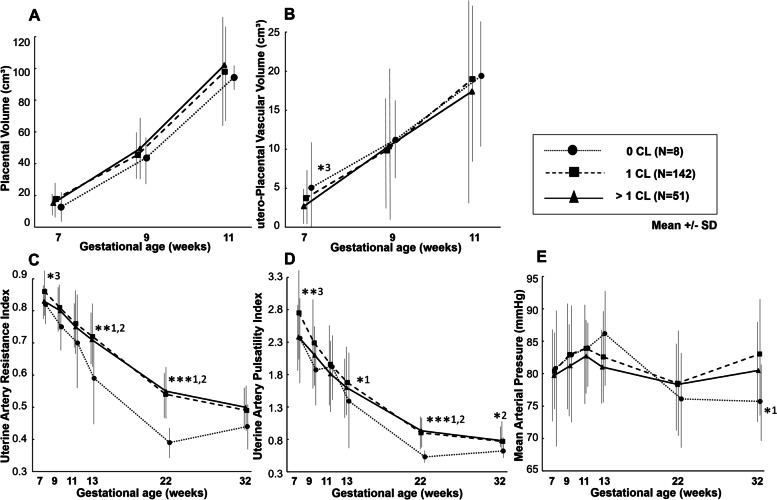
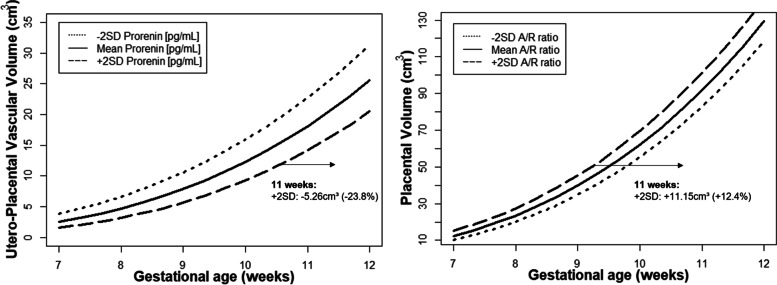
Pregnancies without a CL show lower uterine artery indices throughout gestation than 1 CL and > 1 CL pregnancies, while parameters of placental development are comparable among the CL groups. After adjustment for patient- and treatment-related factors, first-trimester prorenin concentrations are positively associated with uterine artery pulsatility and resistance indices (β 0.06, 95% CI 0.01;0.12, p = 0.04 and β 0.10, 95% CI 0.01;0.20, p = 0.04, respectively), while high prorenin concentrations are negatively associated with first-trimester utero-placental vascular volume (β -0.23, 95% CI -0.44;-0.02, p = 0.04) and placental weight (β -93.8, 95%CI -160.3;-27.4, p = 0.006). In contrast, the aldosterone/renin ratio is positively associated with first-trimester placental volume (β 0.12, 95% CI 0.01;0.24, p = 0.04).
The absence of a CL, resulting in low prorenin concentrations, associates with low uterine artery pulsatility and resistance, while high prorenin concentrations associate with a low utero-placental vascular volume and weight. These data support a scenario in which excess prorenin, by upregulating angiotensin II, increases uterine resistance, thereby preventing normal placental (vascular) development, and increasing the risk of small-for-gestational age deliveries. Simultaneously, high aldosterone concentrations, by ensuring volume expansion, exert the opposite.
妊娠时黄体(CL)数量大于 1 个时会出现高动力循环,并增加小于胎龄儿分娩的风险。CL 释放的因子之一是前肾素,它是肾素的无活性前体。由于肾素-血管紧张素-醛固酮系统(RAAS)参与早期血流动力学妊娠适应,我们将 CL 数量和妊娠早期前肾素浓度(作为 RAAS 活性的指标)以及醛固酮/肾素比值(作为血管紧张素非依赖性醛固酮作用的指标)与从妊娠早期开始纵向测量的子宫胎盘(血管)发育的非侵入性标志物联系起来。
从鹿特丹围孕期队列中选择了 201 名自然受孕或体外受精治疗后怀孕的女性(0(n=8)、1(n=143)或>1(n=51)个 CL)。在妊娠 11 周时测定母体 RAAS 成分。在妊娠 7、9 和 11 周时通过经阴道 3D 超声扫描测量胎盘体积和子宫胎盘血管体积,在妊娠 7、9、11、13、22 和 32 周时通过脉冲波多普勒超声评估子宫动脉搏动和阻力指数。出生时使用标准化程序获得胎盘重量。
无 CL 的妊娠子宫动脉指数在整个妊娠期间均低于 1 个 CL 和>1 个 CL 的妊娠,而胎盘发育参数在 CL 组之间是可比的。调整患者和治疗相关因素后,妊娠早期前肾素浓度与子宫动脉搏动和阻力指数呈正相关(β 0.06,95%CI 0.01;0.12,p=0.04 和β 0.10,95%CI 0.01;0.20,p=0.04),而高前肾素浓度与妊娠早期子宫胎盘血管体积(β -0.23,95%CI -0.44;-0.02,p=0.04)和胎盘重量(β -93.8,95%CI -160.3;-27.4,p=0.006)呈负相关。相比之下,醛固酮/肾素比值与妊娠早期胎盘体积呈正相关(β 0.12,95%CI 0.01;0.24,p=0.04)。
CL 缺失导致前肾素浓度降低,与子宫动脉搏动和阻力降低相关,而高前肾素浓度与子宫胎盘血管体积和重量降低相关。这些数据支持这样一种情况,即过量的前肾素通过上调血管紧张素 II 增加子宫阻力,从而阻止正常的胎盘(血管)发育,并增加小于胎龄儿分娩的风险。同时,高醛固酮浓度通过确保体积扩张产生相反的作用。