Department of Cardiology, Dijon University Hospital, 14 rue Paul Gaffarel, Dijon, 21079, France.
Department of Cardiology, Referral Center for Cardiac Amyloidosis, GRC Amyloid Research Institute, DHU-ATVB, Inserm U955, University Hospital Henri Mondor, Créteil, France.
ESC Heart Fail. 2022 Feb;9(1):740-750. doi: 10.1002/ehf2.13663. Epub 2021 Nov 3.
Cardiac resynchronization therapy (CRT) is highly effective in dilated cardiomyopathy (DCM) patients with impaired left ventricular ejection fraction (LVEF) and left bundle block branch. In cardiac amyloidosis (CA) patients, left ventricular dysfunction and conduction defects are common, but the potential of CRT to improve cardiac remodelling and survival in this particular setting remains undefined. We investigated cardiovascular outcomes in CA patients after CRT implantation in terms of CRT echocardiographic response and major cardiovascular events (MACEs).
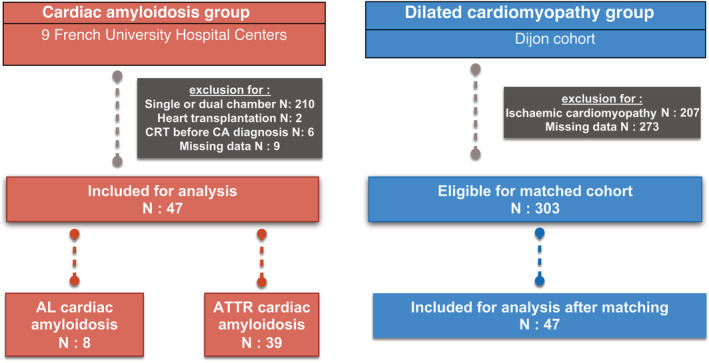
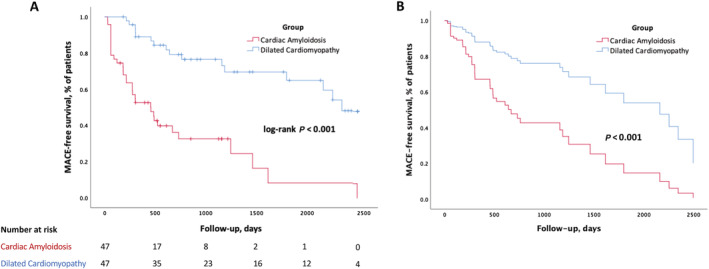
Our retrospective study included 47 CA patients implanted with CRT devices from January 2012 to February 2020, in nine French university hospitals (77 ± 6 years old, baseline LVEF 30 ± 8%) compared with propensity-matched (1:1 for age, LVEF at implantation, and CRT indication) DCM patients with a CRT device. CA patients had lower rates of CRT response (absolute delta LVEF ≥ 10%) compared with DCM patients (36% vs. 70%, P = 0.002). After multivariate Cox analysis, CA was independently associated with MACE (hospitalization for heart failure/cardiovascular death) [hazard ratio (HR) 3.73, 95% confidence interval (CI) 1.85-7.54, P < 0.001], along with the absence of CRT response (HR 3.01, 95% CI 1.56-5.79, P = 0.001). The presence of echocardiographic CRT response (absolute delta LVEF ≥ 10%) was the only predictive factor of MACE-free survival in CA patients (HR 0.36, 95% CI 0.15-0.86, P = 0.002).
Compared with a matched cohort of DCM patients, CA patients had a lower rate of CRT response and consequently a worse cardiovascular prognosis after CRT implantation. However, CRT could be beneficial even in CA patients given that CRT response was associated with better cardiac outcomes in this population.
心脏再同步治疗(CRT)在左心室射血分数(LVEF)降低和左束支传导阻滞的扩张型心肌病(DCM)患者中具有显著疗效。在心脏淀粉样变性(CA)患者中,左心室功能障碍和传导缺陷很常见,但 CRT 在这种特殊情况下改善心脏重构和生存率的潜力尚未确定。我们研究了 CRT 植入后 CA 患者的心血管结局,包括 CRT 超声心动图反应和主要心血管事件(MACE)。
我们的回顾性研究纳入了 2012 年 1 月至 2020 年 2 月在法国 9 所大学医院植入 CRT 设备的 47 例 CA 患者(77±6 岁,基线 LVEF 30±8%),并与 1:1 年龄匹配(植入时 LVEF 和 CRT 适应证)的 DCM 患者进行比较。与 DCM 患者相比,CA 患者 CRT 反应率(绝对 LVEF 差值≥10%)较低(36% vs. 70%,P=0.002)。多变量 Cox 分析后,CA 独立与 MACE(因心力衰竭/心血管死亡住院)相关(风险比[HR]3.73,95%置信区间[CI]1.85-7.54,P<0.001),与 CRT 无反应相关(HR 3.01,95% CI 1.56-5.79,P=0.001)。存在超声心动图 CRT 反应(绝对 LVEF 差值≥10%)是 CA 患者无 MACE 生存的唯一预测因素(HR 0.36,95% CI 0.15-0.86,P=0.002)。
与 DCM 患者匹配队列相比,CA 患者 CRT 反应率较低,因此 CRT 植入后心血管预后较差。然而,即使在 CA 患者中,CRT 也可能有益,因为 CRT 反应与该人群的心脏结局改善相关。