Department of Pediatrics, Boston University School of Medicine (LE Marcil, B Zuckerman, RJ Vinci), Boston, Mass.
Department of Pediatrics, Dell Medical School, The University of Texas at Austin (ML Hole, L Rosen, MB Bennett), Austin, Tex.
Acad Pediatr. 2021 Nov-Dec;21(8S):S169-S176. doi: 10.1016/j.acap.2021.03.017.
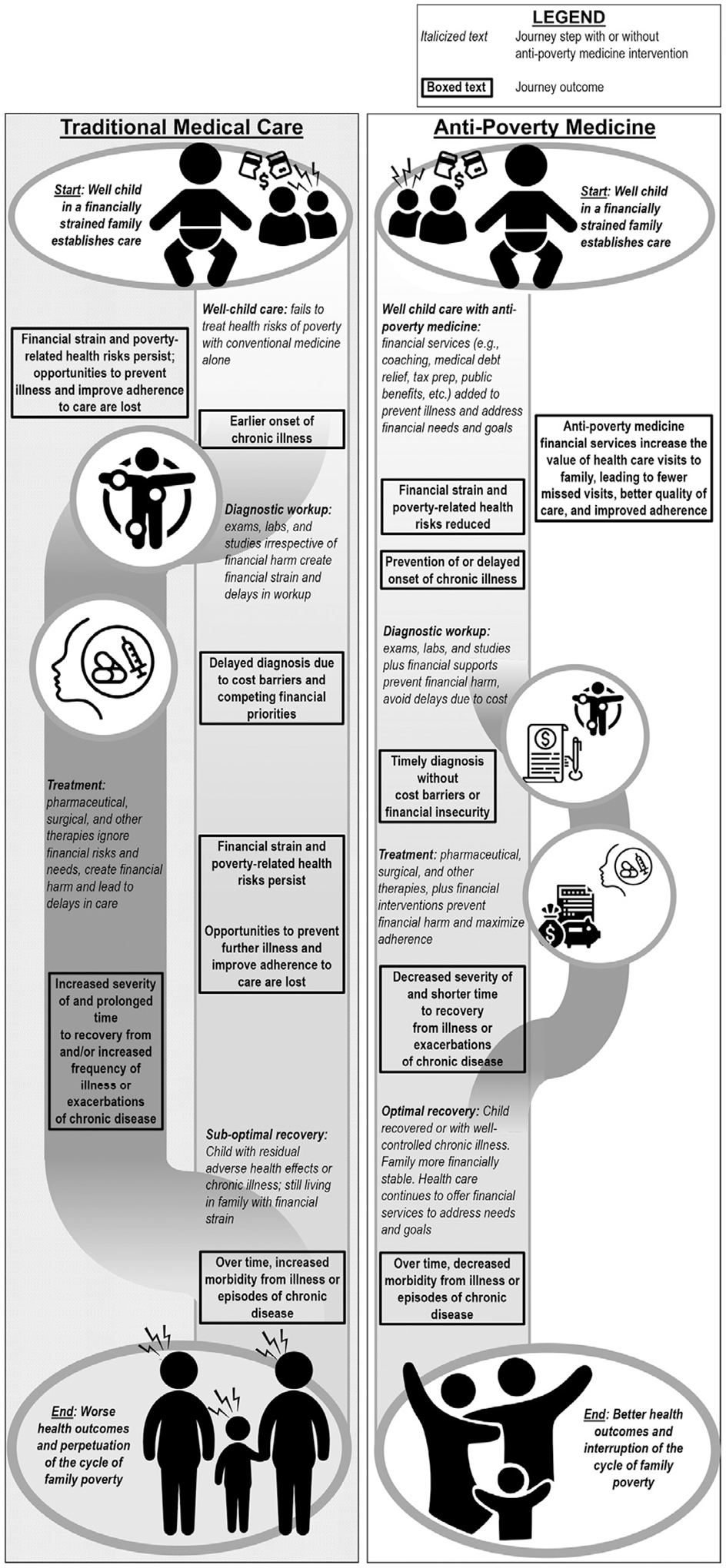
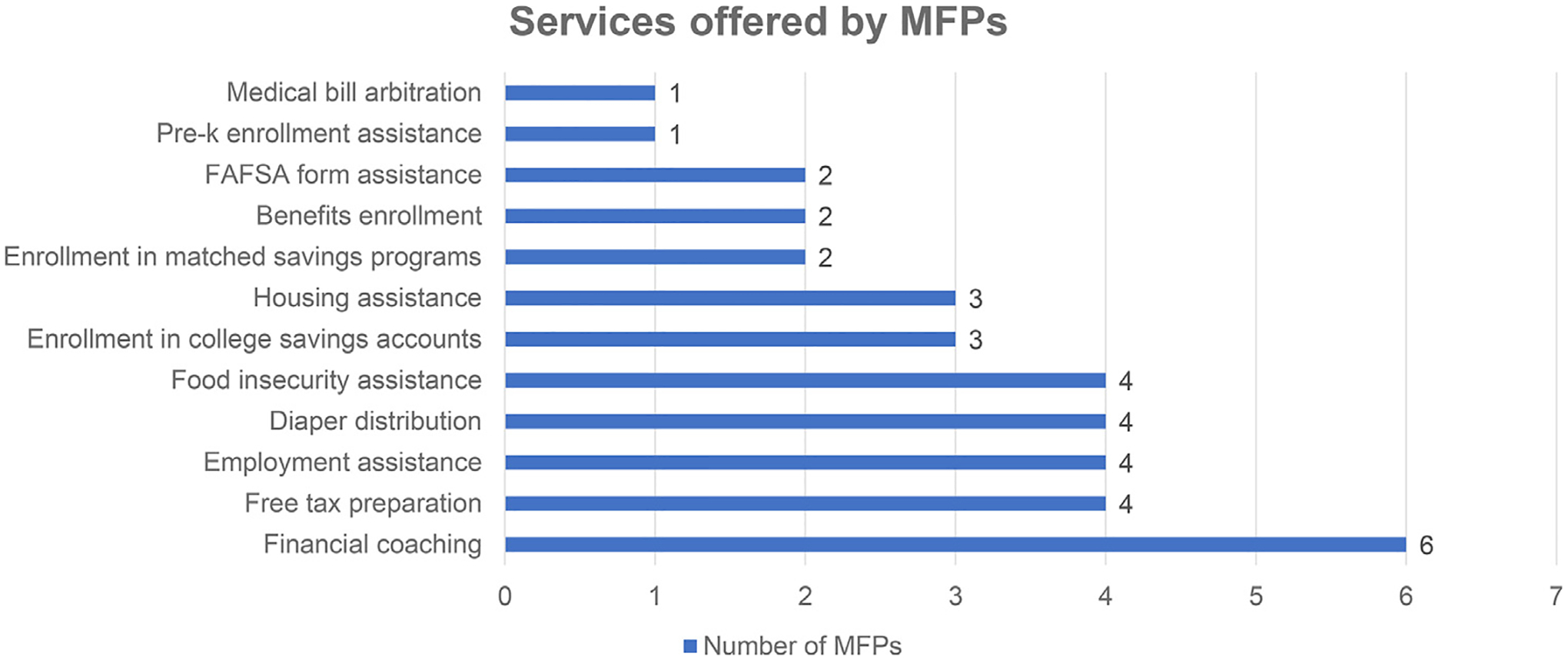
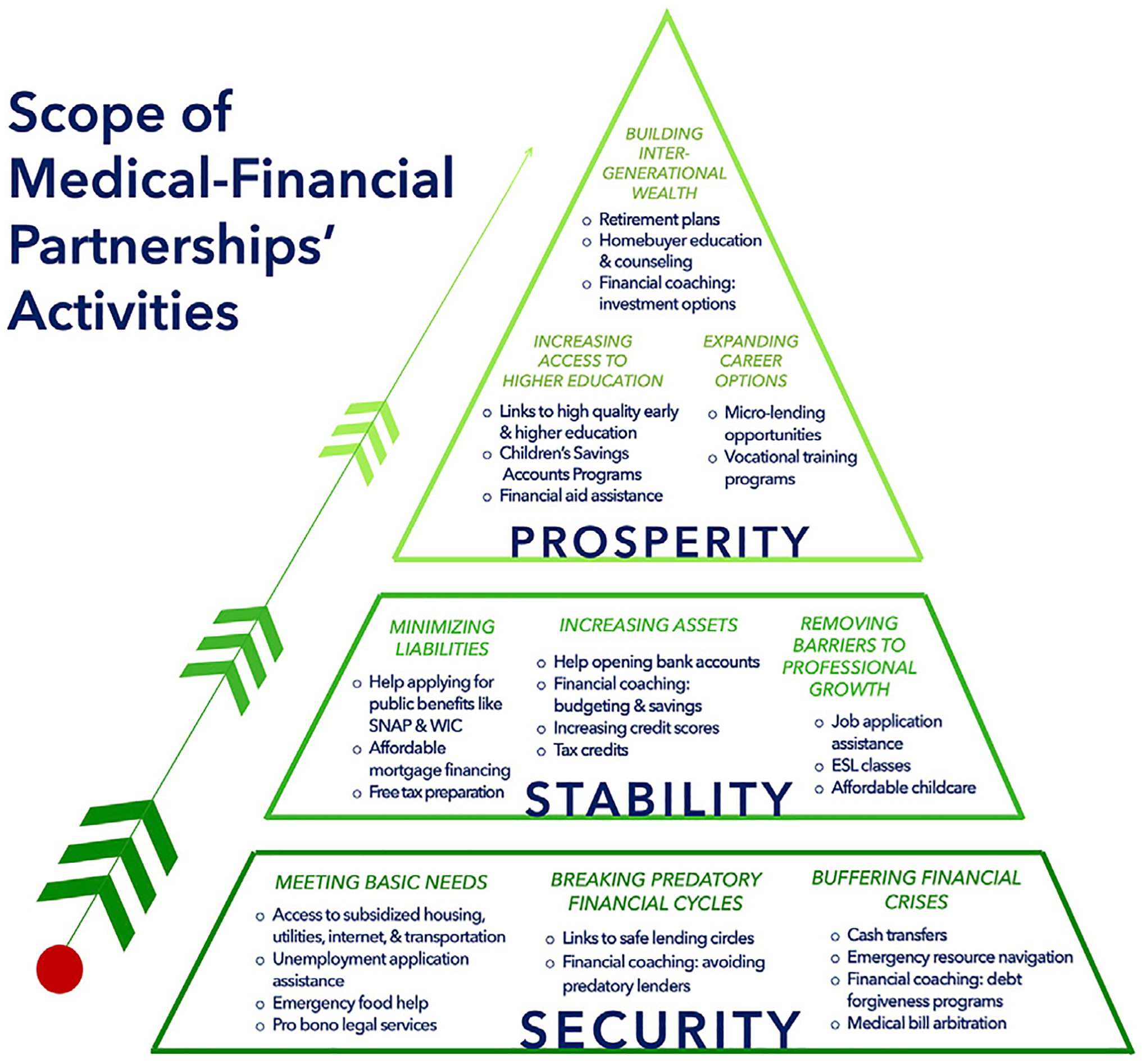
Poverty threatens child health. In the United States, financial strain, which encompasses income and asset poverty, is common with many complex etiologies. Even relatively successful antipoverty programs and policies fall short of serving all families in need, endangering health. We describe a new approach to address this pervasive health problem: antipoverty medicine. Historically, medicine has viewed poverty as a social problem outside of its scope. Increasingly, health care has addressed poverty's downstream effects, such as food and housing insecurity. However, strong evidence now shows that poverty affects biology, and thus, merits treatment as a medical problem. A new approach uses Medical-Financial Partnerships (MFPs), in which healthcare systems and financial service organizations collaborate to improve health by reducing family financial strain. MFPs help families grow assets by increasing savings, decreasing debt, and improving credit and economic opportunity while building a solid foundation for lifelong financial, physical, and mental health. We review evidence-based approaches to poverty alleviation, including conditional and unconditional cash transfers, savings vehicles, debt relief, credit repair, financial coaching, and employment assistance. We describe current national MFPs and highlight different applications of these evidence-based clinical financial interventions. Current MFP models reveal implementation opportunities and challenges, including time and space constraints, time-sensitive processes, lack of familiarity among patients and communities served, and sustainability in traditional medical settings. We conclude that pediatric health care practices can intervene upon poverty and should consider embracing antipoverty medicine as an essential part of the future of pediatric care.
贫困威胁儿童健康。在美国,经济压力(包括收入贫困和资产贫困)普遍存在,病因复杂。即使是相对成功的扶贫项目和政策也无法满足所有有需要的家庭,从而危及健康。我们描述了一种解决这一普遍存在的健康问题的新方法:扶贫医学。历史上,医学将贫困视为其范畴之外的社会问题。越来越多的医疗保健已经解决了贫困的下游影响,如食品和住房不安全问题。然而,现在有强有力的证据表明,贫困会影响生物学,因此,将其视为医疗问题进行治疗是合理的。一种新方法是利用医疗-金融伙伴关系(MFPs),即医疗系统和金融服务组织合作,通过减少家庭经济压力来改善健康。MFPs 通过增加储蓄、减少债务、改善信用和经济机会来帮助家庭增加资产,同时为终生的财务、身体和心理健康打下坚实的基础。我们回顾了扶贫的循证方法,包括有条件和无条件现金转移、储蓄工具、债务减免、信用修复、财务指导和就业援助。我们描述了当前的国家 MFPs,并强调了这些循证临床金融干预措施的不同应用。当前的 MFP 模型揭示了实施机会和挑战,包括时间和空间限制、时间敏感的流程、服务对象的患者和社区缺乏熟悉度以及在传统医疗环境中的可持续性。我们得出结论,儿科医疗保健实践可以干预贫困问题,并应考虑将扶贫医学作为儿科保健未来的重要组成部分。