Univ. Lille, Inserm U1172 LilNCog, CHU Lille, FHU Precise, Lille, France.
Hospital Clínico San Carlos, Madrid, Spain.
Eur J Neurol. 2022 Mar;29(3):790-801. doi: 10.1111/ene.15171. Epub 2021 Nov 25.
Using the treatment goal of "no evidence of disease activity" (NEDA) incorporating magnetic resonance imaging (MRI) re-baselining, we aimed to assess the efficacy of ocrelizumab in patients with relapsing-remitting multiple sclerosis with a prior suboptimal response, defined by MRI or relapse criteria, to one or two disease-modifying therapies (DMTs).
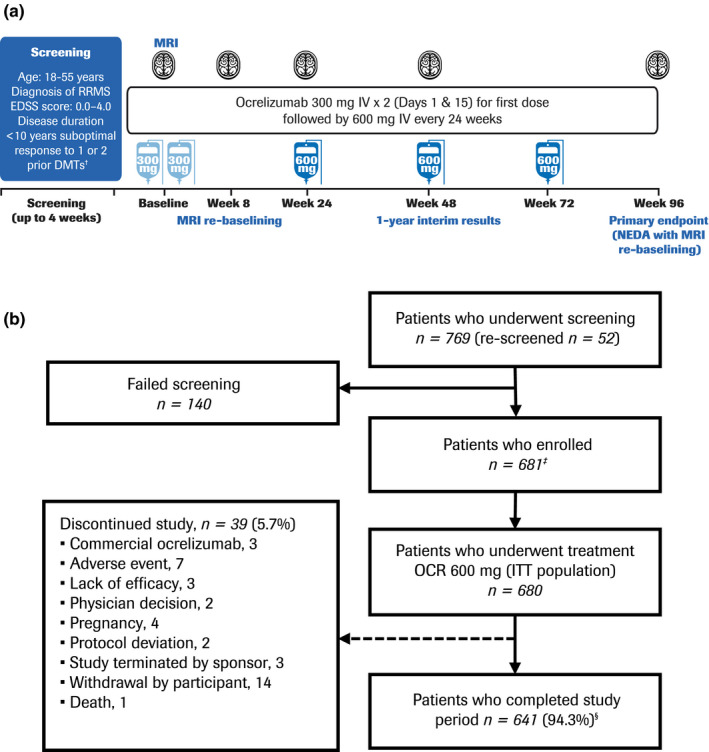
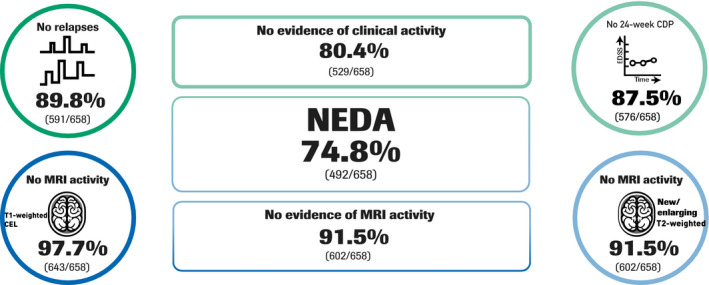
CASTING was a prospective, international, multicenter, single-arm, open-label phase 3 trial (NCT02861014). Patients (Expanded Disability Status Scale [EDSS] score ≤ 4.0, with discontinued prior DMT of ≥6 months duration due to suboptimal disease control) received intravenous ocrelizumab 600 mg every 24 weeks for 96 weeks. The primary endpoint was NEDA (defined as absence of relapses, disability progression, and inflammatory MRI measures, with prespecified MRI re-baselining at Week 8) over 96 weeks.
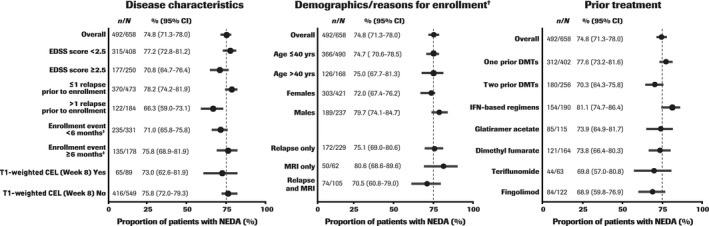
A total of 680 patients were enrolled, 167 (24.6%) based on MRI activity only. At Week 96, 74.8% (95% confidence interval [CI] 71.3-78.0, n/N = 492/658) of patients had NEDA. NEDA was highest among patients enrolled due to MRI activity alone (80.6% [95% CI 68.6-89.6], n/N = 50/62) versus those enrolled for relapse (75.1% [95% CI 69.0-80.6], n/N = 172/229) or for relapse with MRI (70.5% [95% CI 60.0-79.0], n/N = 74/105). NEDA across subgroups was highest in patients with a baseline EDSS score <2.5 (77.2% [95% CI 72.8-81.2], n/N = 315/408). NEDA was higher in patients receiving one prior DMT (77.6% [95% CI 73.2-81.6], n/N = 312/402) versus two prior DMTs (70.3% [95% CI 64.3-75.8], n/N = 180/256).
In patients switching therapy due to suboptimal disease control, treatment with ocrelizumab led to an overall high NEDA rate across a wide range of disease-related and demographic subgroups, regardless of prior treatment background, with no new safety signals detected.
采用包含磁共振成像(MRI)重新基线的“无疾病活动证据”(NEDA)治疗目标,我们旨在评估奥瑞珠单抗在先前对一种或两种疾病修正疗法(DMT)出现 MRI 或复发标准定义的不充分反应(经治疗后疾病控制不佳而停药)的复发缓解型多发性硬化患者中的疗效。
CASTING 是一项前瞻性、国际性、多中心、单臂、开放标签的 3 期试验(NCT02861014)。患者(扩展残疾状态量表 [EDSS]评分≤4.0,先前的 DMT 因治疗后疾病控制不佳而停药≥6 个月)接受每 24 周静脉注射奥瑞珠单抗 600mg,共 96 周。主要终点为 96 周时的 NEDA(定义为无复发、残疾进展和炎症性 MRI 指标,同时在第 8 周进行预设的 MRI 重新基线)。
共纳入 680 例患者,其中 167 例(24.6%)仅基于 MRI 活动。第 96 周时,74.8%(95%置信区间 [CI] 71.3-78.0,n/N=492/658)的患者达到了 NEDA。仅基于 MRI 活动而纳入的患者(80.6%[95%CI 68.6-89.6,n/N=50/62])与因复发(75.1%[95%CI 69.0-80.6,n/N=172/229)或因复发和 MRI(70.5%[95%CI 60.0-79.0,n/N=74/105)而纳入的患者相比,NEDA 更高。基线 EDSS 评分<2.5 的患者(n/N=315/408)NEDA 最高(77.2%[95%CI 72.8-81.2])。与接受两种先前 DMT 相比(n/N=180/256),接受一种先前 DMT 的患者(n/N=312/402)NEDA 更高(77.6%[95%CI 73.2-81.6])。
在因治疗后疾病控制不佳而转换治疗的患者中,奥瑞珠单抗治疗总体上导致了广泛的疾病相关和人口统计学亚组的高 NEDA 率,无论先前的治疗背景如何,均未发现新的安全性信号。