Nasr Ayman O, Al-Harbi Turki Muslih, AlRamadan Fatimah Sami
Department of Surgery, King Fahad Hospital Of University-Collage of Medicine, Imam Abdulrahman Bin Faisal University, Saudi Arabia.
Collage of Medicine, Imam Abdulrahman Bin Faisal University, Saudi Arabia.
Int J Surg Case Rep. 2021 Nov;88:106547. doi: 10.1016/j.ijscr.2021.106547. Epub 2021 Nov 2.
Blunt carotid injury (BCI) injury is a rare sequel of trauma and could result in ischemic complication if not detected and treated early. The presence of high-grade solid organ injury with ongoing bleeding represents additional challenge in treating BCI.
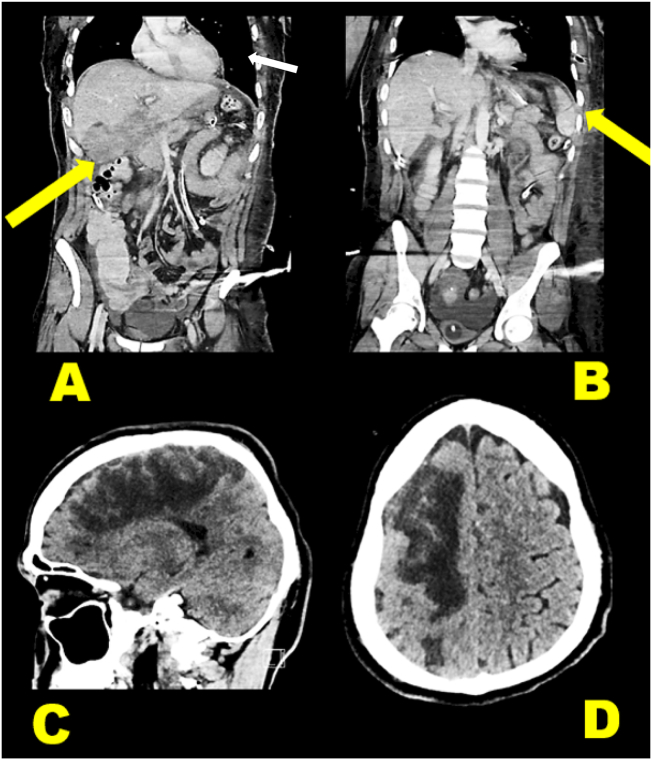
A 25-year-old victim of motor vehicle collision resulted in grade IV liver, grade III left kidney and grade I spleen injury. He underwent an urgent laparotomy with transient liver packing at local hospital. A full body Contrast-Enhanced Computer Tomography (CECT) upon arrival revealed right internal carotid intimal tear with intra and extra-cranial thrombosis and a 3 cm aneurysm. With a decreased level of consciousness, the patient showed a GCS of 13 and left-sided hemiplegia. After complex multidisciplinary treatment sessions, patient recovered with a partial regain of left-sided muscle power.
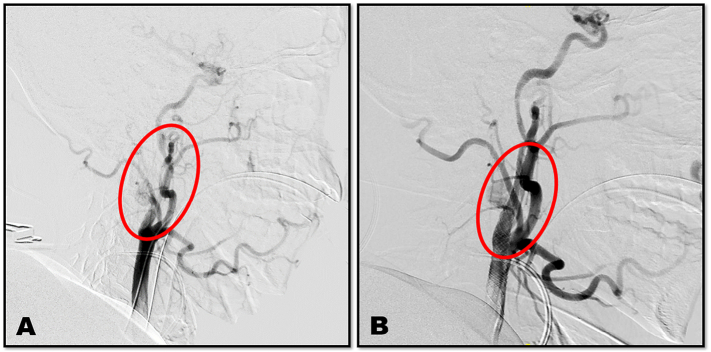
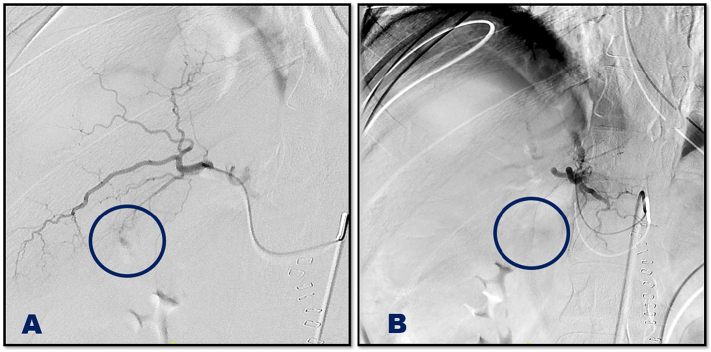
Selective embolization of active liver bleeding was a turning point in the management of our patient as it deferred the need for a second operative intervention. It was a necessary step before endovascular stenting and recanalization of the BCI to restore the circulation to the right cerebral hemisphere. Dual anti-platelet therapy (DAPT) was necessary to prevent thrombosis of the stent and continuity of carotid recanalization.
BCI with traumatic ischaemic hemiplegia associating a sum of life-threatening multiple injuries including high grade liver trauma with ongoing bleeding could still be managed non-operatively with acceptable outcome in the presence of a comprehensive specialized multidisciplinary service.
钝性颈动脉损伤(BCI)是创伤后罕见的后遗症,若不及早发现和治疗,可能导致缺血性并发症。存在伴有持续出血的高级别实体器官损伤给BCI的治疗带来了额外挑战。
一名25岁的机动车碰撞受害者,导致IV级肝损伤、III级左肾损伤和I级脾损伤。他在当地医院接受了紧急剖腹手术并进行了临时肝脏填塞。到达时的全身对比增强计算机断层扫描(CECT)显示右颈内动脉内膜撕裂,伴有颅内和颅外血栓形成以及一个3厘米的动脉瘤。患者意识水平下降,格拉斯哥昏迷量表(GCS)评分为13分,左侧偏瘫。经过多学科综合治疗,患者康复,左侧肌肉力量部分恢复。
对活动性肝出血进行选择性栓塞是我们患者治疗中的一个转折点,因为它推迟了二次手术干预的必要性。这是在对BCI进行血管内支架置入和再通以恢复右大脑半球血液循环之前的必要步骤。双重抗血小板治疗(DAPT)对于预防支架血栓形成和颈动脉再通的连续性是必要的。
伴有创伤性缺血性偏瘫的BCI,合并包括伴有持续出血的高级别肝外伤在内的一系列危及生命的多发伤,在有全面专业的多学科服务的情况下,仍可通过非手术治疗获得可接受的结果。