Department of Public Health and Primary Care, Leiden University Medical Center, room V6.26, Postbus 9600 2300, RC, Leiden, The Netherlands.
Hadoks (Elzha), President Kennedylaan 15, 2517, JK, The Hague, The Netherlands.
BMC Health Serv Res. 2021 Nov 9;21(1):1218. doi: 10.1186/s12913-021-07198-2.
Dutch standard diabetes care is generally protocol-driven. However, considering that general practices wish to tailor diabetes care to individual patients and encourage self-management, particularly in light of current COVID-19 related constraints, protocols and other barriers may hinder implementation. The impact of dispensing with protocol and implementation of self-management interventions on patient monitoring and experiences are not known. This study aims to evaluate tailoring of care by understanding experiences of well-organised practices 1) when dispensing with protocol; 2) determining the key conditions for successful implementation of self-management interventions; and furthermore exploring patients' experiences regarding dispensing with protocol and self-management interventions.
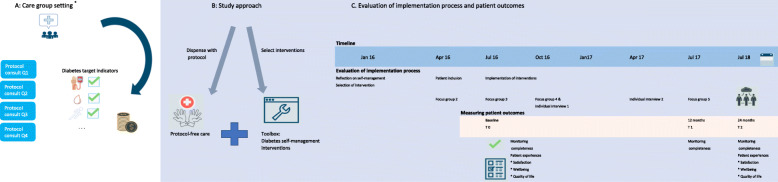
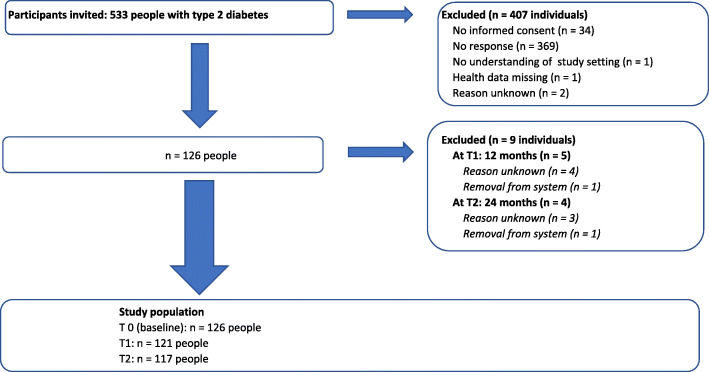
in this mixed-methods prospective study, practices (n = 49) were invited to participate if they met protocol-related quality targets, and their adult patients with well-controlled type 2 diabetes were invited if they had received protocol-based diabetes care for a minimum of 1 year. For practices, study participation consisted of the opportunity to deliver protocol-free diabetes care, with selection and implementation of self-management interventions. For patients, study participation provided exposure to protocol-free diabetes care and self-management interventions. Qualitative outcomes (practices: 5 focus groups, 2 individual interviews) included experiences of dispensing with protocol and the implementation process of self-management interventions, operationalised as implementation fidelity. Quantitative outcomes (patients: routine registry data, surveys) consisted of diabetes monitoring completeness, satisfaction, wellbeing and health status at baseline and follow-up (24 months).
Qualitative: In participating practices (n = 4), dispensing with protocol encouraged reflection on tailored care and selection of various self-management interventions A focus on patient preferences, team collaboration and intervention feasibility was associated with high implementation fidelity Quantitative: In patients (n = 126), likelihood of complete monitoring decreased significantly after two years (OR 0.2 (95% CI 0.1-0.5), p < 0.001) Satisfaction decreased slightly (- 1.6 (95% CI -2.6;-0.6), p = 0.001) Non-significant declines were found in wellbeing (- 1.3 (95% CI -5.4; 2.9), p = 0.55) and health status (- 3.0 (95% CI -7.1; 1.2), p = 0.16).
To tailor diabetes care to individual patients within well-organised practices, we recommend dispensing with protocol while maintaining one structural annual monitoring consultation, combined with the well-supported implementation of feasible self-management interventions. Interventions should be selected and delivered with the involvement of patients and should involve population preferences and solid team collaborations.
荷兰标准的糖尿病护理通常是基于方案的。然而,考虑到一般实践希望根据个体患者的情况调整糖尿病护理,并鼓励自我管理,特别是考虑到当前与 COVID-19 相关的限制,方案和其他障碍可能会阻碍实施。放弃方案和实施自我管理干预对患者监测和体验的影响尚不清楚。本研究旨在通过了解组织良好的实践 1)在放弃方案时的护理调整情况;2)确定成功实施自我管理干预的关键条件;并进一步探讨患者对放弃方案和自我管理干预的体验,来评估护理的调整。
在这项混合方法前瞻性研究中,如果实践符合与方案相关的质量目标,并且其成年 2 型糖尿病患者接受了至少 1 年的基于方案的糖尿病护理,则邀请这些实践参与研究。对于实践,研究参与包括提供无方案的糖尿病护理的机会,并选择和实施自我管理干预。对于患者,研究参与提供了无方案的糖尿病护理和自我管理干预的体验。定性结果(实践:5 个焦点小组,2 个个人访谈)包括放弃方案和自我管理干预实施过程的体验,实施的忠实度作为操作化指标。定量结果(患者:常规登记数据,调查)包括基线和随访(24 个月)时的糖尿病监测完整性、满意度、幸福感和健康状况。
定性:在参与的实践中(n=4),放弃方案鼓励对量身定制的护理和各种自我管理干预的反思,重点关注患者的偏好、团队合作和干预的可行性与高实施忠实度相关。定量:在患者中(n=126),两年后完全监测的可能性显著下降(OR 0.2(95%CI 0.1-0.5),p<0.001),满意度略有下降(-1.6(95%CI -2.6;-0.6),p=0.001),幸福感没有显著下降(-1.3(95%CI -5.4;2.9),p=0.55),健康状况也没有显著下降(-3.0(95%CI -7.1;1.2),p=0.16)。
为了在组织良好的实践中为个体患者量身定制糖尿病护理,我们建议在保持一次结构性年度监测咨询的同时放弃方案,同时结合可行的自我管理干预的有力支持。干预措施应在患者的参与下进行选择和提供,并应涉及人群偏好和稳固的团队合作。