Public Health and Primary Care, Leiden University Medical Center, Leiden, The Netherlands.
HADOKS (ELZHA), The Hague, The Netherlands.
BMJ Open. 2019 Mar 13;9(3):e027208. doi: 10.1136/bmjopen-2018-027208.
Management of type 2 diabetes mellitus (T2DM) requires frequent monitoring of patients. Within a collective care group setting, doubts on the clinical effects of registration are a barrier for full adoption of T2DM registration in general practice. We explored whether full monitoring of biomedical and lifestyle-related target indicators within a care group approach is associated with lower HbA levels.
Observational, real-life cohort study.
Primary care data registry from the Hadoks (EerstelijnsZorggroepHaaglanden) care group.
The care group provides general practitioners collectively with organisational support to facilitate structured T2DM primary care. Patients are offered quarterly medical and lifestyle-related consultation.
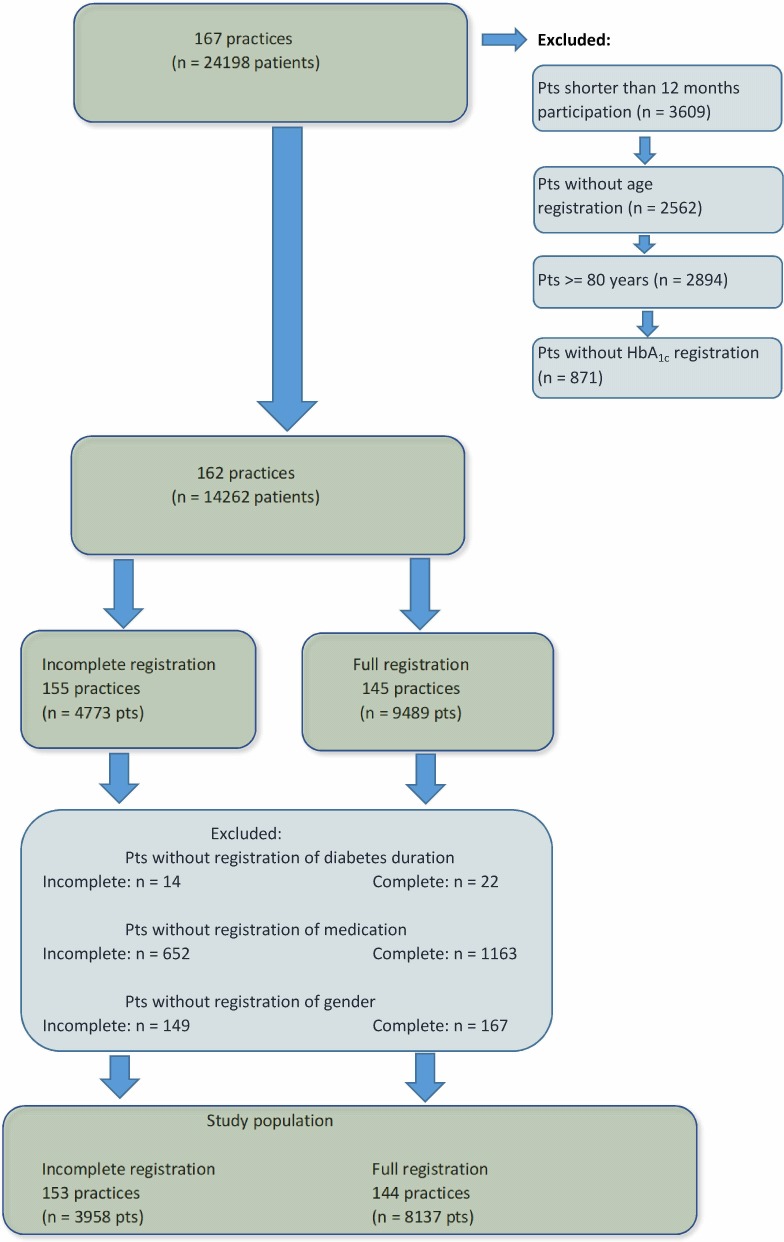
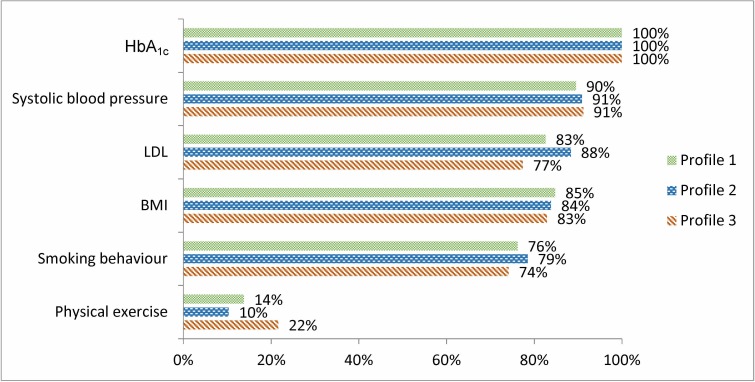
Full monitoring of each target indicator in patients with T2DM which includes minimally one measure of HbA level, systolic blood pressure, LDL, BMI, smoking behaviour and physical exercise between January and December 2014; otherwise, patients were defined as 'incompletely monitored'. HbA levels of 8137 fully monitored and 3958 incompletely monitored patients were compared, adjusted for the confounders diabetes duration, age and gender. Since recommended HbA values depend on age, medication use and diabetes duration, analyses were stratified into three HbA profile groups. Linear multilevel analyses enabled adjustment for general practice.
Compared with incompletely monitored patients, fully monitored patients had significantly lower HbA levels (95% CI) in the first (-2.03 [-2.53 to -1.52] mmol/mol) (-0.19% [-0.23% to -0.14%]), second (-3.36 [-5.28 to -1.43] mmol/mol) (-0.31% [-0.48% to -0.13%]) and third HbA profile group (-1.89 [-3.76 to -0.01] mmol/mol) (-0.17% [-0.34% to 0.00%]).
CONCLUSIONS/INTERPRETATION: This study shows that in a care group setting, fully monitored patients had significantly lower HbA levels compared with incompletely monitored patients. Since this difference might have considerable clinical impact in terms of T2DM-related risks, this might help general practices in care group settings to overcome barriers on adequate registration and thus improve structured T2DM primary care. From population health management perspective, we recommend a systematic approach to adjust the structured care protocol for incompletely monitored subgroups.
2 型糖尿病(T2DM)的管理需要频繁监测患者。在集体护理组环境中,对注册临床效果的怀疑是普遍采用一般实践中 T2DM 注册的障碍。我们探讨了在护理组方法中全面监测生物医学和与生活方式相关的目标指标是否与较低的 HbA 水平相关。
观察性、真实队列研究。
来自 Hadoks(EerstelijnsZorggroepHaaglanden)护理组的初级保健数据登记处。
护理组为全科医生提供集体组织支持,以促进结构化的 T2DM 初级保健。患者每季度接受一次医疗和与生活方式相关的咨询。
2014 年 1 月至 12 月期间,T2DM 患者的每个目标指标均进行全面监测,至少包括一次 HbA 水平、收缩压、LDL、BMI、吸烟行为和体育锻炼的测量;否则,患者被定义为“监测不完全”。比较了 8137 名充分监测和 3958 名不完全监测患者的 HbA 水平,调整了糖尿病持续时间、年龄和性别等混杂因素。由于推荐的 HbA 值取决于年龄、药物使用和糖尿病持续时间,因此对三个 HbA 特征组进行了分析。线性多层分析使一般实践的调整成为可能。
与监测不完全的患者相比,充分监测的患者 HbA 水平显著降低(95%置信区间):第一组(-2.03[-2.53 至-1.52]mmol/mol)(-0.19%[-0.23%至-0.14%]),第二组(-3.36[-5.28 至-1.43]mmol/mol)(-0.31%[-0.48%至-0.13%])和第三组 HbA 特征组(-1.89[-3.76 至-0.01]mmol/mol)(-0.17%[-0.34%至 0.00%])。
结论/解释:本研究表明,在护理组环境中,与监测不完全的患者相比,充分监测的患者 HbA 水平显著降低。由于这一差异在 T2DM 相关风险方面可能具有相当大的临床影响,这可能有助于护理组环境中的一般实践克服适当登记的障碍,从而改善结构化的 T2DM 初级保健。从人群健康管理的角度来看,我们建议系统地调整结构化护理方案,以适应监测不完全的亚组。