Department of Medical & Molecular Genetics, King's College London, London, UK.
Social, Genetic and Developmental Psychiatry Centre, King's College London, London, UK.
Genome Med. 2021 Nov 9;13(1):180. doi: 10.1186/s13073-021-00994-9.
Cardiorespiratory fitness (CRF) and physical activity (PA) are well-established predictors of morbidity and all-cause mortality. However, CRF is not routinely measured and PA not routinely prescribed as part of standard healthcare. The American Heart Association (AHA) recently presented a scientific case for the inclusion of CRF as a clinical vital sign based on epidemiological and clinical observation. Here, we leverage genetic data in the UK Biobank (UKB) to strengthen the case for CRF as a vital sign and make a case for the prescription of PA.
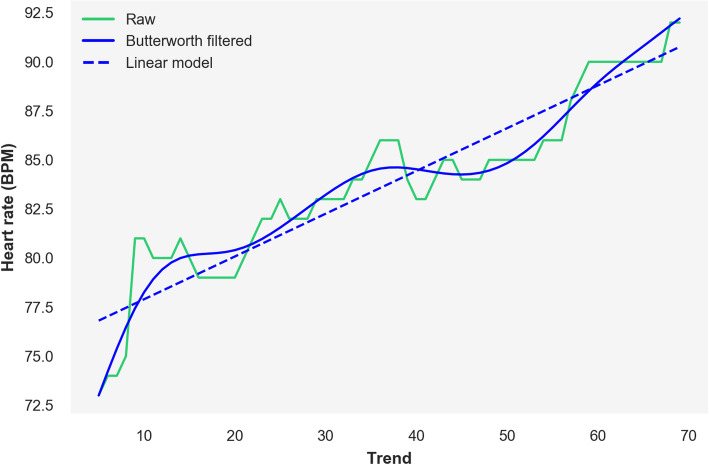
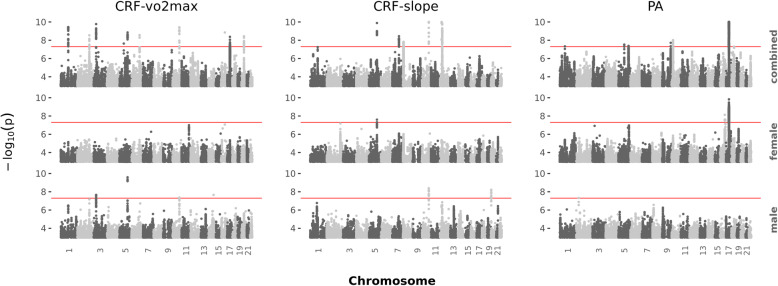
We derived two CRF measures from the heart rate data collected during a submaximal cycle ramp test: CRF-vo2max, an estimate of the participants' maximum volume of oxygen uptake, per kilogram of body weight, per minute; and CRF-slope, an estimate of the rate of increase of heart rate during exercise. Average PA over a 7-day period was derived from a wrist-worn activity tracker. After quality control, 70,783 participants had data on the two derived CRF measures, and 89,683 had PA data. We performed genome-wide association study (GWAS) analyses by sex, and post-GWAS techniques to understand genetic architecture of the traits and prioritise functional genes for follow-up.
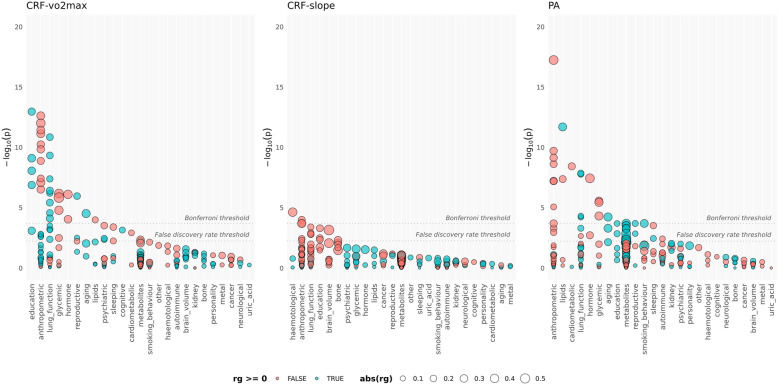
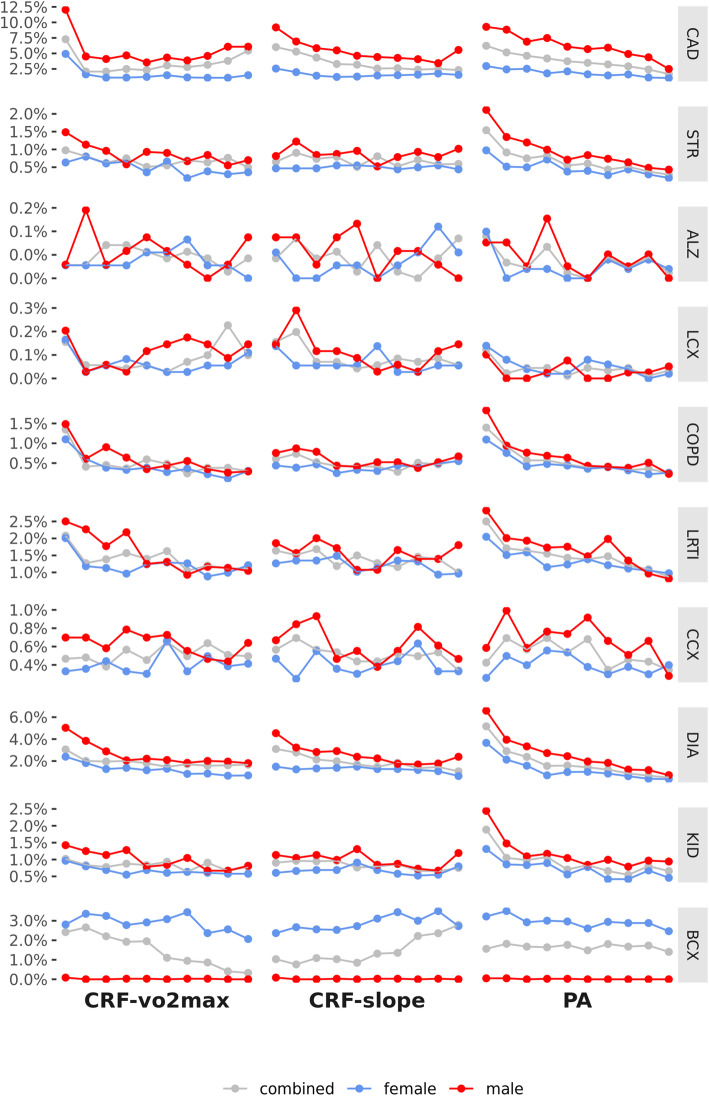
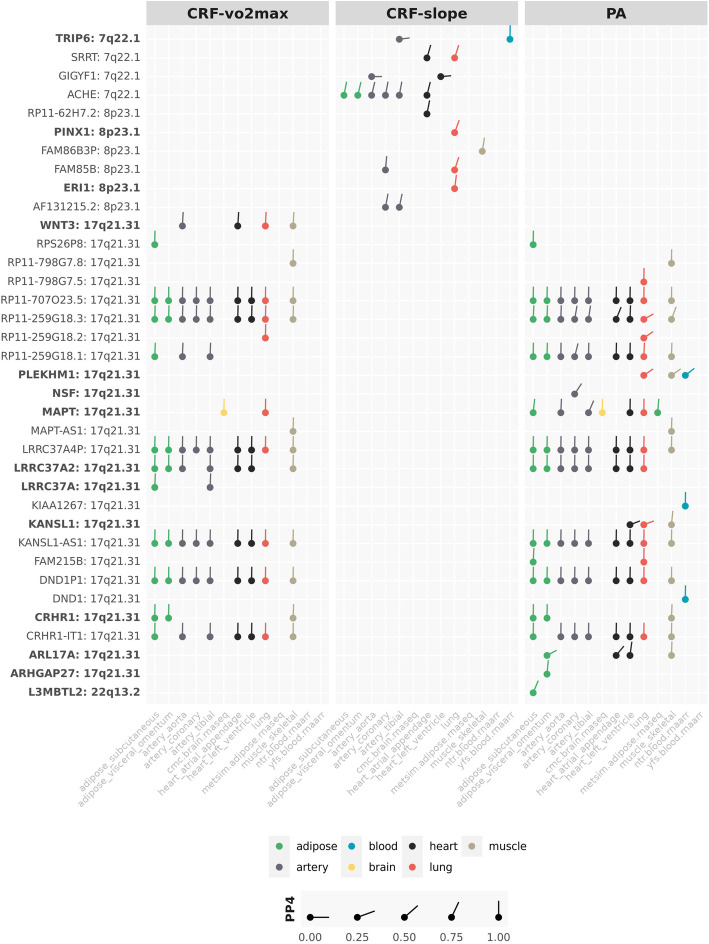
We found strong evidence that genetic variants associated with CRF and PA influenced genetic expression in a relatively small set of genes in the heart, artery, lung, skeletal muscle and adipose tissue. These functionally relevant genes were enriched among genes known to be associated with coronary artery disease (CAD), type 2 diabetes (T2D) and Alzheimer's disease (three of the top 10 causes of death in high-income countries) as well as Parkinson's disease, pulmonary fibrosis, and blood pressure, heart rate, and respiratory phenotypes. Genetic variation associated with lower CRF and PA was also correlated with several disease risk factors (including greater body mass index, body fat and multiple obesity phenotypes); a typical T2D profile (including higher insulin resistance, higher fasting glucose, impaired beta-cell function, hyperglycaemia, hypertriglyceridemia); increased risk for CAD and T2D; and a shorter lifespan.
Genetics supports three decades of evidence for the inclusion of CRF as a clinical vital sign. Given the genetic, clinical and epidemiological evidence linking CRF and PA to increased morbidity and mortality, regular measurement of CRF as a marker of health and routine prescription of PA could be a prudent strategy to support public health.
心肺适能(CRF)和身体活动(PA)是发病率和全因死亡率的可靠预测因素。然而,CRF 并未常规测量,PA 也未常规作为标准医疗保健的一部分进行开处。美国心脏协会(AHA)最近提出了将 CRF 作为临床生命体征的科学依据,这是基于流行病学和临床观察的结果。在这里,我们利用英国生物库(UKB)中的遗传数据来加强 CRF 作为生命体征的依据,并提出 PA 处方的理由。
我们从亚最大强度自行车测试期间收集的心率数据中得出了两个 CRF 指标:CRF-vo2max,参与者每公斤体重每分钟最大耗氧量的估计值;CRF-slope,运动时心率增加率的估计值。在 7 天期间的平均 PA 是从手腕佩戴的活动追踪器中得出的。经过质量控制,有 70783 名参与者有两个衍生的 CRF 指标的数据,89683 名参与者有 PA 数据。我们按性别进行了全基因组关联研究(GWAS)分析,并进行了 GWAS 后技术分析,以了解这些特征的遗传结构,并为后续研究确定功能基因。
我们发现强有力的证据表明,与 CRF 和 PA 相关的遗传变异影响了心脏、动脉、肺、骨骼肌和脂肪组织中相对较小一组基因的基因表达。这些具有功能相关性的基因在与冠心病(CAD)、2 型糖尿病(T2D)和阿尔茨海默病(高收入国家十大死因中的三种)以及帕金森病、肺纤维化和血压、心率和呼吸表型相关的基因中富集。与较低的 CRF 和 PA 相关的遗传变异也与多种疾病风险因素(包括更大的体重指数、体脂肪和多种肥胖表型)相关;典型的 T2D 特征(包括更高的胰岛素抵抗、更高的空腹血糖、β细胞功能受损、高血糖、高甘油三酯血症);CAD 和 T2D 风险增加;以及寿命缩短。
遗传学为将 CRF 作为临床生命体征纳入提供了三十年来的证据支持。鉴于 CRF 和 PA 与发病率和死亡率增加相关的遗传、临床和流行病学证据,定期测量 CRF 作为健康标志物和常规开具 PA 处方可能是支持公共健康的明智策略。