Department of Infectious Diseases, Huashan Hospital, Fudan University, Shanghai, 200040, China.
Department of Infectious Diseases, First Affiliated Hospital of Wannan Medical College, Wuhu, 241000, China.
BMC Gastroenterol. 2021 Nov 10;21(1):422. doi: 10.1186/s12876-021-02007-w.
Although the Asian Pacific Association for the Study of the Liver acute-on-chronic liver failure (ACLF) research consortium (AARC) ACLF score is easy to use in patients with hepatitis b virus-related ACLF (HBV-ACLF), serum lactate is not routinely tested in primary hospitals, and its value may be affected by some interference factors. Neutrophil-to-lymphocyte ratio (NLR) is used to assess the status of bacterial infection (BI) or outcomes in patients with various diseases. We developed an NLR-based AARC ACLF score and compared it with the existing model.
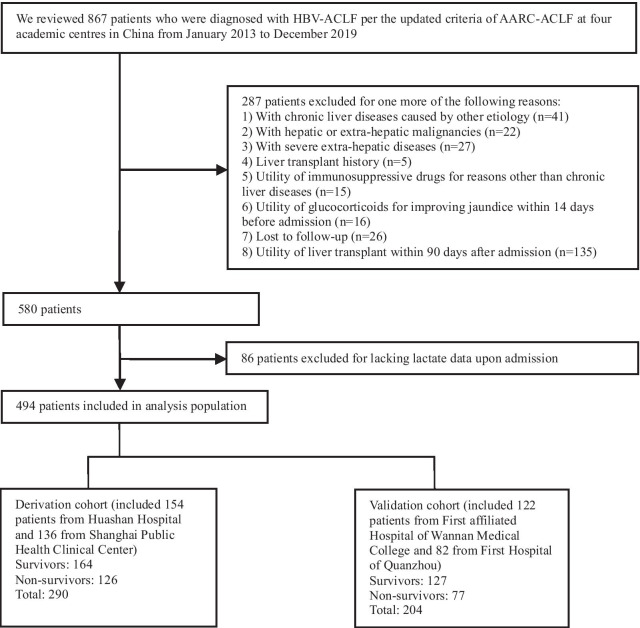
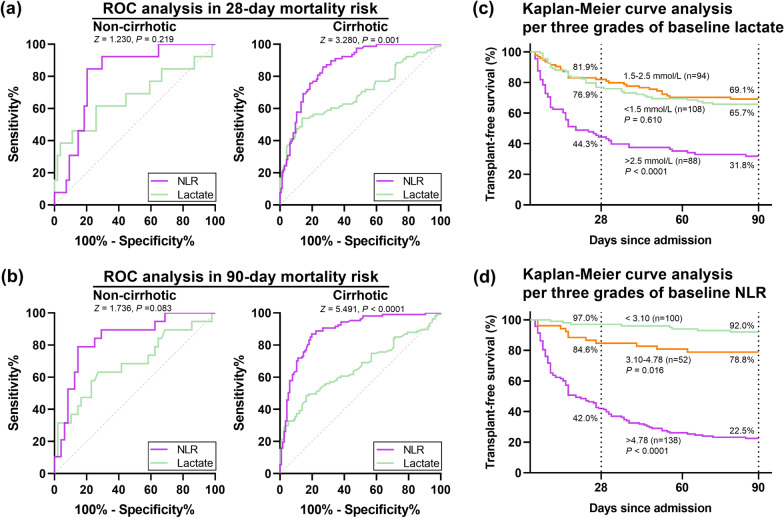
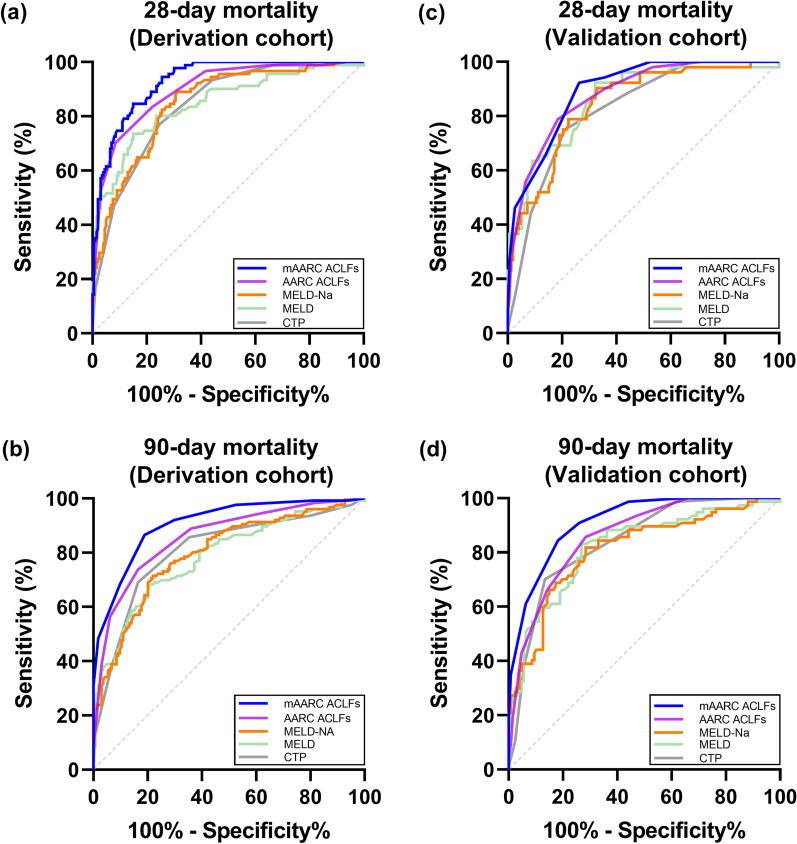
A total of 494 HBV-ACLF patients, enrolled in four tertiary academic hospitals in China with 90-day follow-up, were analysed. Prognostic performance of baseline NLR and lactate were compared between cirrhotic and non-cirrhotic subgroups via the receiver operating curve and Kaplan-Meier analyses. A modified AARC ACLF (mAARC ACLF) score using NLR as a replacement for lactate was developed (n = 290) and validated (n = 204).
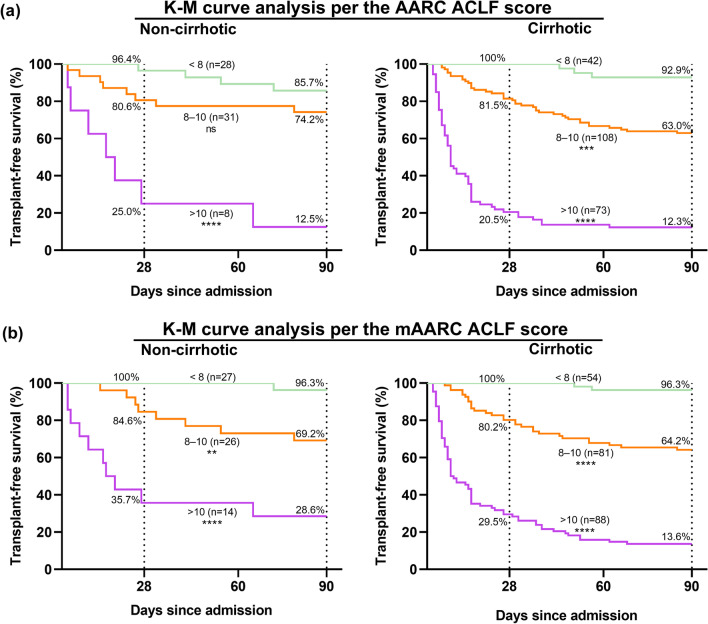
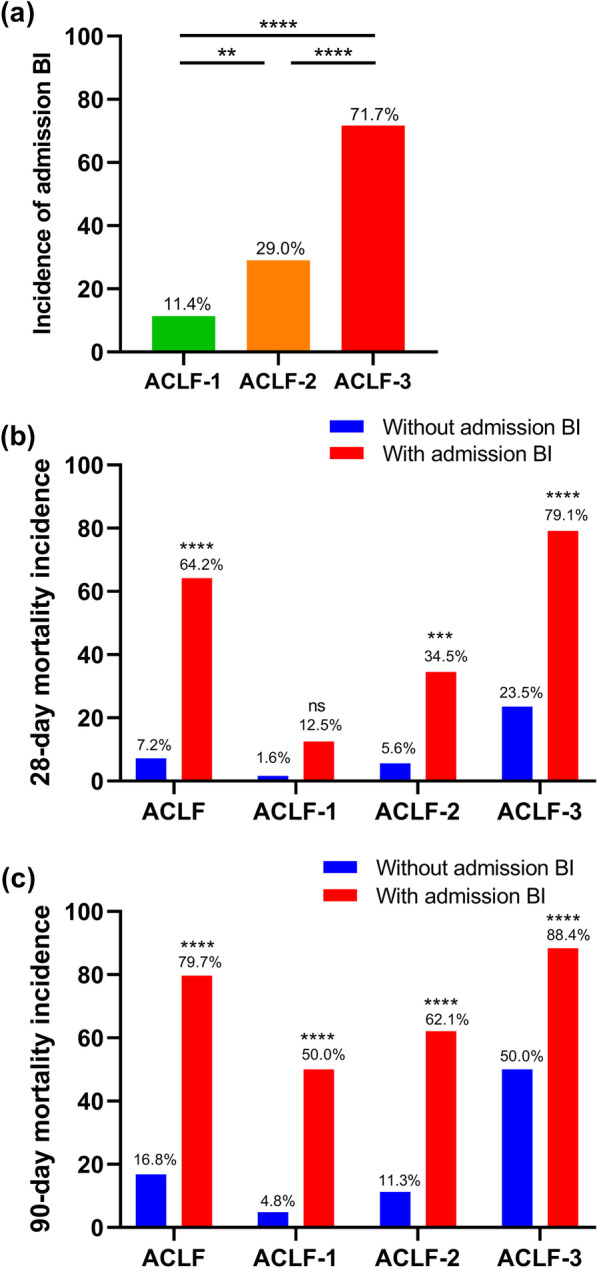
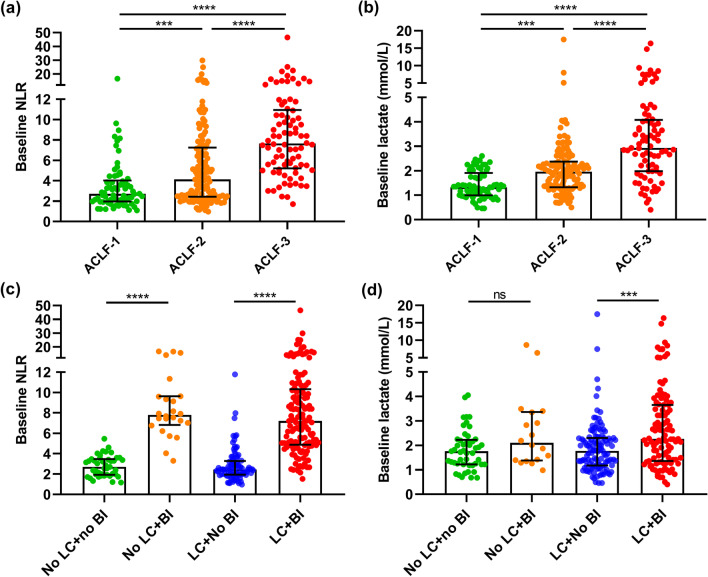
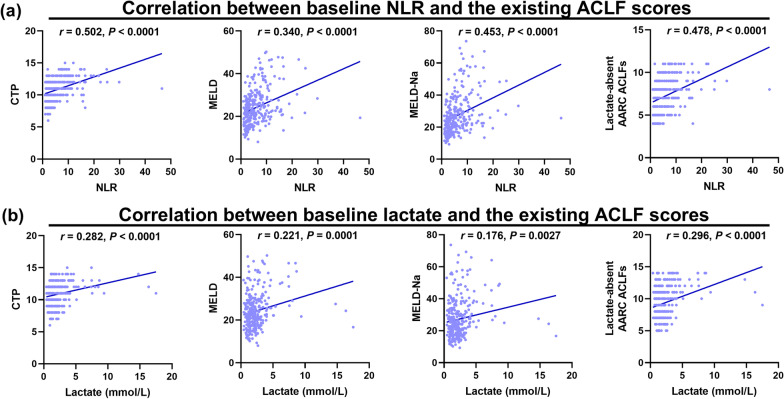
There were significantly higher baseline values of NLR in non-survivors, patients with admission BI, and those with higher grades of ACLF compared with the control groups. Compared with lactate, NLR better reflected BI status in the cirrhotic subgroup, and was more significantly correlated with CTP, MELD, MELD-Na, and the AARC score. NLR was an independent predictor of 90-day mortality, and was categorized into three risk grades (< 3.10, 3.10-4.78, and > 4.78) with 90-day cumulative mortalities of 8%, 21.2%, and 77.5% in the derivation cohort, respectively. The mAARC ACLF score, using the three grades of NLR instead of corresponding levels of lactate, was superior to the other four scores in predicting 90-day mortality in the derivation (AUROC 0.906, 95% CI 0.872-0.940, average P < 0.001) and validation cohorts (AUROC 0.913, 95% CI 0.876-0.950, average P < 0.01), with a considerable performance in predicting 28-day mortality in the two cohorts.
The prognostic value of NLR is superior to that of lactate in predicting short-term mortality risk in cirrhotic and non-cirrhotic patients with HBV-ACLF. NLR can be incorporated into the AARC ACLF scoring system for improving its prognostic accuracy and facilitating the management guidance in patients with HBV-ACLF in primary hospitals.
尽管亚太肝脏研究学会(APASL)急性肝衰竭联盟(ACLF)慢性肝脏衰竭(ACLF)研究联盟(AARC)ACLF 评分易于在乙型肝炎病毒相关 ACLF(HBV-ACLF)患者中使用,但乳酸在基层医院中并未常规检测,其价值可能受到一些干扰因素的影响。中性粒细胞与淋巴细胞比值(NLR)用于评估各种疾病患者的细菌感染(BI)或结局。我们开发了一种基于 NLR 的 AARC ACLF 评分,并与现有模型进行了比较。
共纳入中国 4 家三级学术医院的 494 例 HBV-ACLF 患者,进行 90 天随访。通过接受者操作曲线和 Kaplan-Meier 分析比较 NLR 和乳酸在肝硬化和非肝硬化亚组中基线值与预测短期死亡率的价值。使用 NLR 替代乳酸开发改良的 AARC ACLF(mAARC ACLF)评分(n=290)并进行验证(n=204)。
与对照组相比,非幸存者、入院时存在 BI 者以及 ACLF 分级较高者的 NLR 基线值显著较高。与乳酸相比,NLR 能更好地反映肝硬化亚组的 BI 状态,与 CTP、MELD、MELD-Na 和 AARC 评分的相关性更强。NLR 是 90 天死亡率的独立预测因子,可分为 3 个风险等级(<3.10、3.10-4.78 和>4.78),在推导队列中,90 天累积死亡率分别为 8%、21.2%和 77.5%。使用 NLR 的三个等级替代相应水平的乳酸的 mAARC ACLF 评分,在推导(AUROC 0.906,95%CI 0.872-0.940,平均 P<0.001)和验证队列(AUROC 0.913,95%CI 0.876-0.950,平均 P<0.01)中,预测 90 天死亡率的效能均优于其他 4 个评分,且在两个队列中均具有良好的预测 28 天死亡率的效能。
在预测肝硬化和非肝硬化 HBV-ACLF 患者短期死亡率风险方面,NLR 的预后价值优于乳酸。NLR 可纳入 AARC ACLF 评分系统,以提高其预后准确性,并为基层医院的 HBV-ACLF 患者提供管理指导。