University of Newcastle, Cancer Signalling Research Group, School of Biomedical Sciences and Pharmacy, College of Health, Medicine & Wellbeing, Callaghan, NSW, Australia.
Hunter Medical Research Institute, Cancer Research Program, New Lambton Heights, NSW, Australia.
Oncogene. 2022 Jan;41(4):461-475. doi: 10.1038/s41388-021-02102-y. Epub 2021 Nov 10.
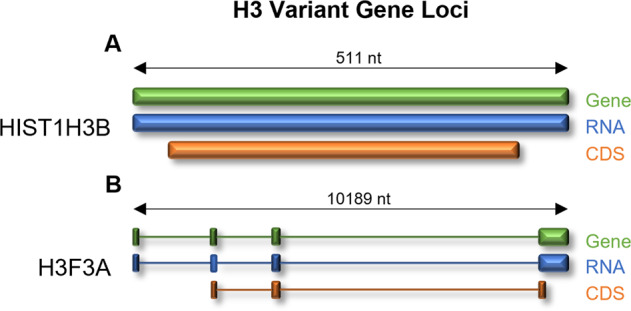
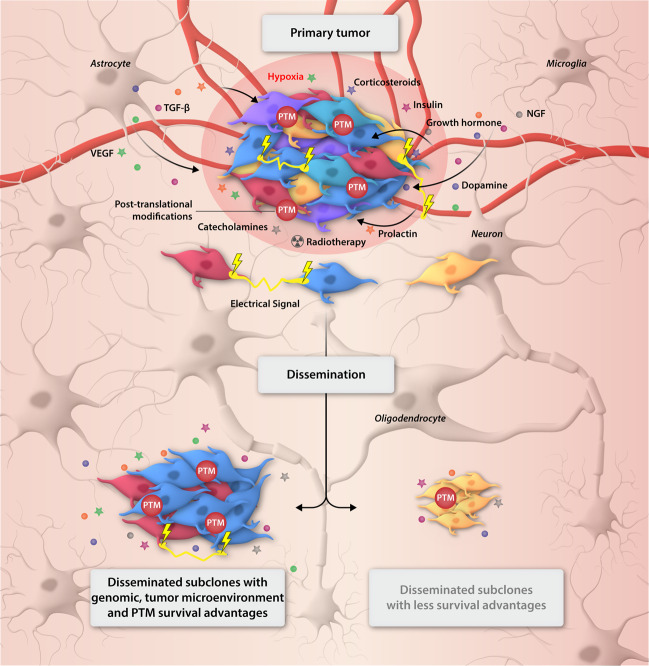
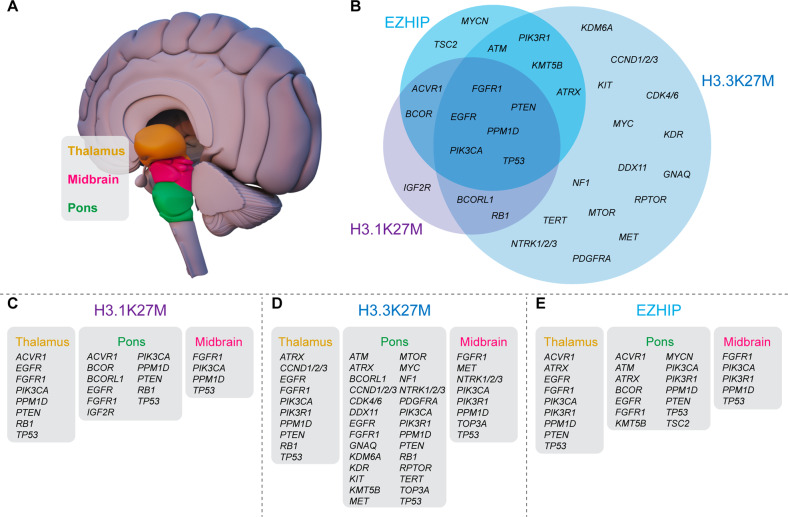
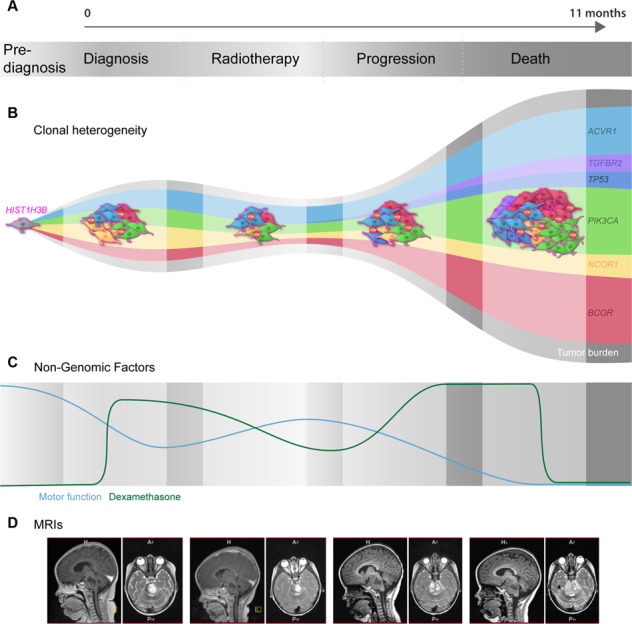
Diffuse midline glioma (DMG) is a deadly pediatric and adolescent central nervous system (CNS) tumor localized along the midline structures of the brain atop the spinal cord. With a median overall survival (OS) of just 9-11-months, DMG is characterized by global hypomethylation of histone H3 at lysine 27 (H3K27me3), driven by recurring somatic mutations in H3 genes including, HIST1H3B/C (H3.1K27M) or H3F3A (H3.3K27M), or through overexpression of EZHIP in patients harboring wildtype H3. The recent World Health Organization's 5th Classification of CNS Tumors now designates DMG as, 'H3 K27-altered', suggesting that global H3K27me3 hypomethylation is a ubiquitous feature of DMG and drives devastating transcriptional programs for which there are no treatments. H3-alterations co-segregate with various other somatic driver mutations, highlighting the high-level of intertumoral heterogeneity of DMG. Furthermore, DMG is also characterized by very high-level intratumoral diversity with tumors harboring multiple subclones within each primary tumor. Each subclone contains their own combinations of driver and passenger lesions that continually evolve, making precision-based medicine challenging to successful execute. Whilst the intertumoral heterogeneity of DMG has been extensively investigated, this is yet to translate to an increase in patient survival. Conversely, our understanding of the non-genomic factors that drive the rapid growth and fatal nature of DMG, including endogenous and exogenous microenvironmental influences, neurological cues, and the posttranscriptional and posttranslational architecture of DMG remains enigmatic or at best, immature. However, these factors are likely to play a significant role in the complex biological sequelae that drives the disease. Here we summarize the heterogeneity of DMG and emphasize how analysis of the posttranslational architecture may improve treatment paradigms. We describe factors that contribute to treatment response and disease progression, as well as highlight the potential for pharmaco-proteogenomics (i.e., the integration of genomics, proteomics and pharmacology) in the management of this uniformly fatal cancer.
弥漫性中线脑胶质瘤(DMG)是一种致命的儿科和青少年中枢神经系统(CNS)肿瘤,位于脊髓上方的脑中线结构内。DMG 的中位总生存期(OS)仅为 9-11 个月,其特征是组蛋白 H3 在赖氨酸 27 处的整体去甲基化(H3K27me3),由 H3 基因的反复体细胞突变驱动,包括 HIST1H3B/C(H3.1K27M)或 H3F3A(H3.3K27M),或通过携带野生型 H3 的患者中 EZHIP 的过表达。最近的世界卫生组织第 5 版中枢神经系统肿瘤分类现在将 DMG 指定为“H3 K27 改变”,这表明全局 H3K27me3 去甲基化是 DMG 的普遍特征,并为其驱动的毁灭性转录程序提供了无治疗方法。H3 改变与各种其他体细胞驱动突变共分离,突出了 DMG 的高度肿瘤间异质性。此外,DMG 还具有非常高水平的肿瘤内异质性,每个原发性肿瘤内都存在多个亚克隆。每个亚克隆都包含自己的驱动和乘客病变组合,这些病变不断进化,使得基于精准的医学治疗难以成功实施。虽然 DMG 的肿瘤间异质性已经得到了广泛的研究,但这并没有转化为患者生存率的提高。相反,我们对驱动 DMG 快速生长和致命性质的非基因组因素的理解,包括内源性和外源性微环境影响、神经提示以及 DMG 的转录后和翻译后结构,仍然很神秘,或者最多是不成熟的。然而,这些因素可能在驱动疾病的复杂生物学后果中发挥重要作用。在这里,我们总结了 DMG 的异质性,并强调了分析翻译后结构如何改善治疗方案。我们描述了导致治疗反应和疾病进展的因素,并强调了 pharmaco-proteogenomics(即基因组学、蛋白质组学和药理学的整合)在管理这种普遍致命癌症中的潜力。