Division of Oncology, Children's Hospital of Philadelphia, Philadelphia, PA.
Section of Transplantation and Cellular Therapy, Children's Hospital Los Angeles Cancer and Blood Disease Institute, Norris Comprehensive Cancer Center, Keck School of Medicine, University of Southern California, Los Angeles, CA.
J Clin Oncol. 2022 Mar 20;40(9):932-944. doi: 10.1200/JCO.21.01405. Epub 2021 Nov 12.
CD19-targeted chimeric antigen receptor T cells (CD19-CAR) and blinatumomab effectively induce remission in relapsed or refractory B-cell acute lymphoblastic leukemia (ALL) but are also associated with CD19 antigen modulation. There are limited data regarding the impact of prior blinatumomab exposure on subsequent CD19-CAR outcomes.
We conducted a multicenter, retrospective review of children and young adults with relapsed or refractory ALL who received CD19-CAR between 2012 and 2019. Primary objectives addressed 6-month relapse-free survival (RFS) and event-free survival (EFS), stratified by blinatumomab use. Secondary objectives included comparison of longer-term survival outcomes, complete remission rates, CD19 modulation, and identification of factors associated with EFS.
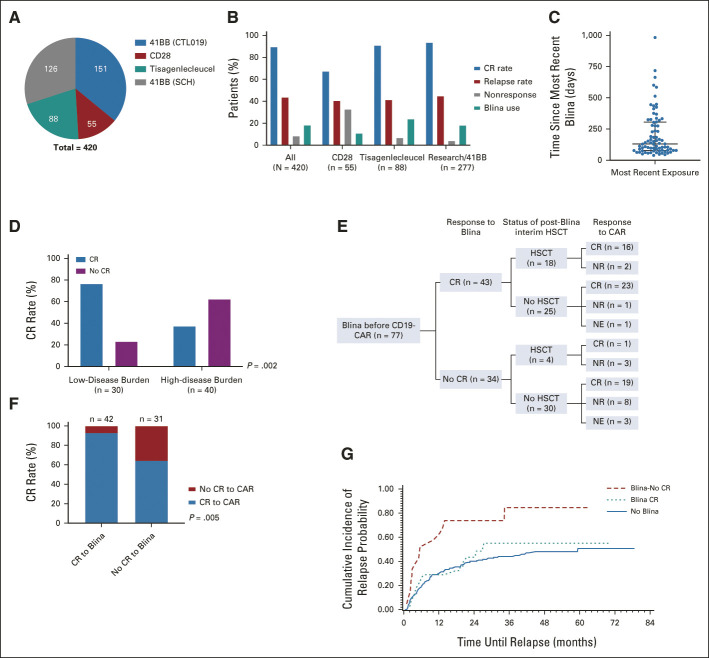
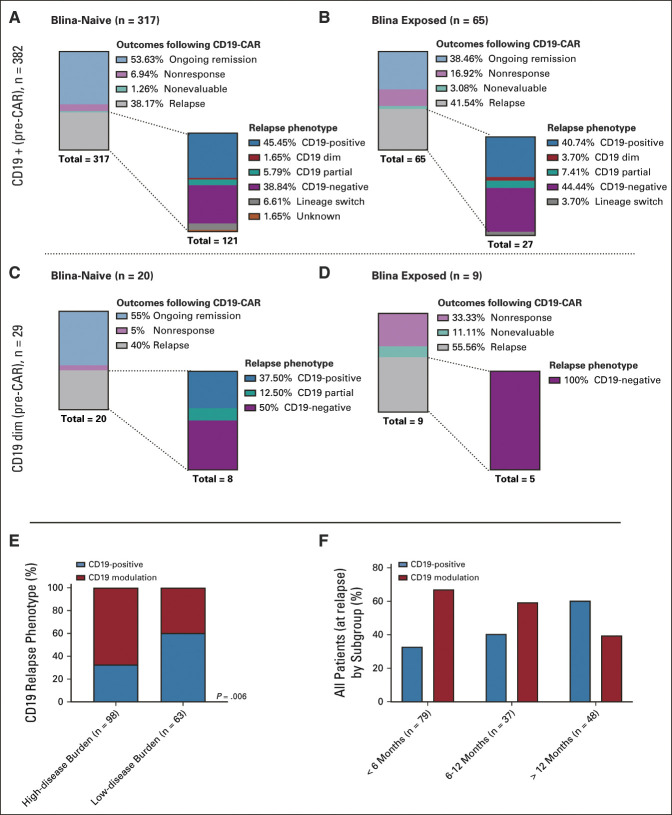
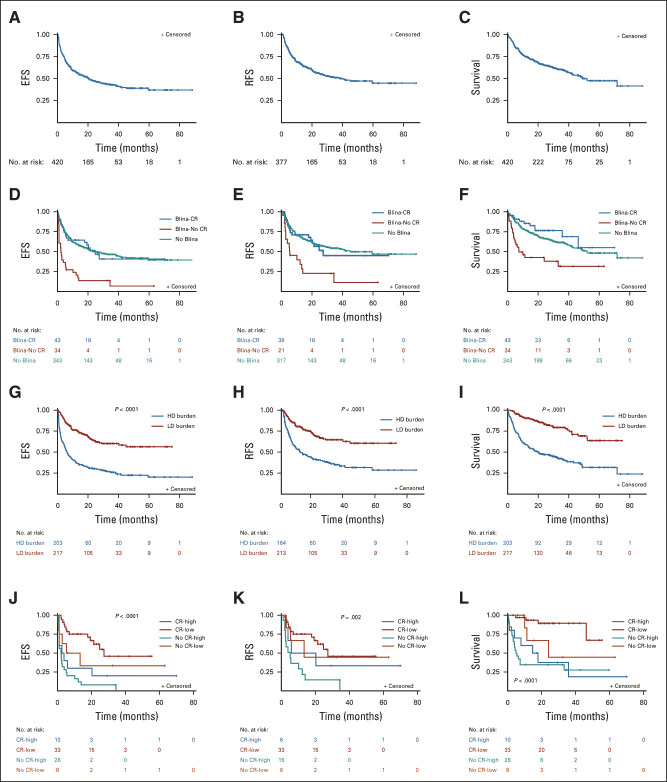
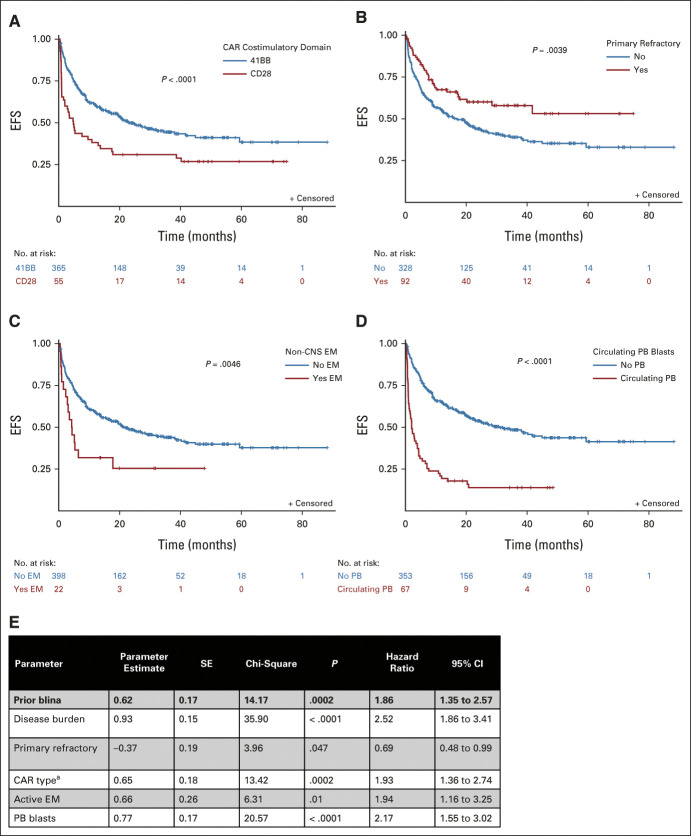
Of 420 patients (median age, 12.7 years; interquartile range, 7.1-17.5) treated with commercial tisagenlecleucel or one of three investigational CD19-CAR constructs, 77 (18.3%) received prior blinatumomab. Blinatumomab-exposed patients more frequently harbored rearrangements and underwent a prior stem-cell transplant than blinatumomab-naïve patients. Among patients evaluable for CD19-CAR response (n = 412), blinatumomab nonresponders had lower complete remission rates to CD19-CAR (20 of 31, 64.5%) than blinatumomab responders (39 of 42, 92.9%) or blinatumomab-naive patients (317 of 339, 93.5%), < .0001. Following CD19-CAR, blinatumomab nonresponders had worse 6-month EFS (27.3%; 95% CI, 13.6 to 43.0) compared with blinatumomab responders (66.9%; 95% CI, 50.6 to 78.9; < .0001) or blinatumomab-naïve patients (72.6%; 95% CI, 67.5 to 77; < .0001) and worse RFS. High-disease burden independently associated with inferior EFS. CD19-dim or partial expression (preinfusion) was more frequently seen in blinatumomab-exposed patients (13.3% 6.5%; = .06) and associated with lower EFS and RFS.
With the largest series to date in pediatric CD19-CAR, and, to our knowledge, the first to study the impact of sequential CD19 targeting, we demonstrate that blinatumomab nonresponse and high-disease burden were independently associated with worse RFS and EFS, identifying important indicators of long-term outcomes following CD19-CAR.
CD19 靶向嵌合抗原受体 T 细胞(CD19-CAR)和blinatumomab 可有效诱导复发或难治性 B 细胞急性淋巴细胞白血病(ALL)缓解,但也与 CD19 抗原调节有关。关于先前blinatumomab 暴露对后续 CD19-CAR 结果的影响,数据有限。
我们对 2012 年至 2019 年间接受 CD19-CAR 治疗的复发或难治性 ALL 儿童和青少年进行了多中心回顾性研究。主要目的是根据 blinatumomab 的使用情况,评估 6 个月无复发生存率(RFS)和无事件生存(EFS)。次要目的包括比较长期生存结果、完全缓解率、CD19 调节以及确定与 EFS 相关的因素。
在接受商业 tisagenlecleucel 或三种研究性 CD19-CAR 构建体之一治疗的 420 名患者中(中位年龄 12.7 岁;四分位间距 7.1-17.5),77 名(18.3%)患者接受过先前的 blinatumomab 治疗。blinatumomab 暴露患者更频繁地携带 重排,并在接受干细胞移植前进行了治疗。在可评估 CD19-CAR 反应的患者中(n=412),blinatumomab 无应答者的 CD19-CAR 完全缓解率(20/31,64.5%)低于 blinatumomab 应答者(39/42,92.9%)或 blinatumomab 初治患者(317/339,93.5%),<.0001。在接受 CD19-CAR 治疗后,blinatumomab 无应答者的 6 个月 EFS 较差(27.3%;95%CI,13.6 至 43.0),与 blinatumomab 应答者(66.9%;95%CI,50.6 至 78.9;<.0001)或 blinatumomab 初治患者(72.6%;95%CI,67.5 至 77;<.0001)相比,6 个月 EFS 较差,RFS 也较差。高疾病负担与较差的 EFS 独立相关。blinatumomab 暴露患者更频繁地出现 CD19 表达减少或部分表达(输注前)(13.3% 6.5%;=.06),与较差的 EFS 和 RFS 相关。
本研究是迄今为止在儿科 CD19-CAR 中最大的系列研究,也是首次研究序贯 CD19 靶向的影响,我们证明了 blinatumomab 无应答和高疾病负担与较差的 RFS 和 EFS 独立相关,确定了 CD19-CAR 后长期结果的重要指标。