Tvedt Tor Henrik Anderson, Vo Anh Khoi, Bruserud Øystein, Reikvam Håkon
Department of Hematology, Oslo University Hospital, 0372 Oslo, Norway.
Department of Clinical Science, University of Bergen, 5020 Bergen, Norway.
J Clin Med. 2021 Nov 6;10(21):5190. doi: 10.3390/jcm10215190.
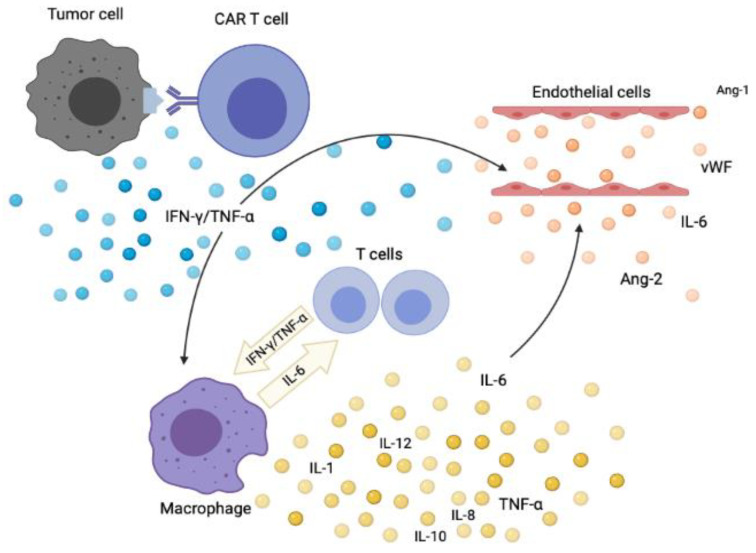
Cytokine release syndrome (CRS) is an acute systemic inflammatory syndrome characterized by fever and multiple organ dysfunction associated with (i) chimeric antigen receptor (CAR)-T cell therapy, (ii) therapeutic antibodies, and (iii) haploidentical allogeneic stem cell transplantation (haplo-allo-HSCT). Severe CRS can be life-threatening in some cases and requires prompt management of those toxicities and is still a great challenge for physicians. The pathophysiology of CRS is still not fully understood, which also applies to the identifications of predictive biomarkers that can forecast these features in advance. However, a broad range of cytokines are involved in the dynamics of CRS. Treatment approaches include both broad spectrum of immunosuppressant, such as corticosteroids, as well as more specific inhibition of cytokine release. In the present manuscript we will try to review an update regarding pathophysiology, etiology, diagnostics, and therapeutic options for this serious complication.
细胞因子释放综合征(CRS)是一种急性全身性炎症综合征,其特征为发热和多器官功能障碍,与以下情况相关:(i)嵌合抗原受体(CAR)-T细胞疗法;(ii)治疗性抗体;(iii)单倍体相合异基因干细胞移植(单倍体异基因造血干细胞移植)。严重的CRS在某些情况下可能危及生命,需要对这些毒性进行及时处理,对医生而言仍然是一个巨大的挑战。CRS的病理生理学仍未完全阐明,这同样适用于能够提前预测这些特征的预测性生物标志物的识别。然而,多种细胞因子参与了CRS的动态变化。治疗方法包括广谱免疫抑制剂,如皮质类固醇,以及更特异性地抑制细胞因子释放。在本手稿中,我们将尝试综述关于这种严重并发症的病理生理学、病因、诊断和治疗选择的最新情况。