Wingerchuk Dean M, Zhang Ina, Kielhorn Adrian, Royston Minying, Levy Michael, Fujihara Kazuo, Nakashima Ichiro, Tanvir Imran, Paul Friedemann, Pittock Sean J
Mayo Clinic, Scottsdale, AZ, USA.
PRECISIONheor, Oakland, CA, USA.
Neurol Ther. 2022 Mar;11(1):123-135. doi: 10.1007/s40120-021-00295-8. Epub 2021 Nov 13.
Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune disease defined by attacks on the central nervous system that cause irreversible damage. Recent approval of NMOSD therapies warrants investigations of comparative efficacy to inform treatment decisions.
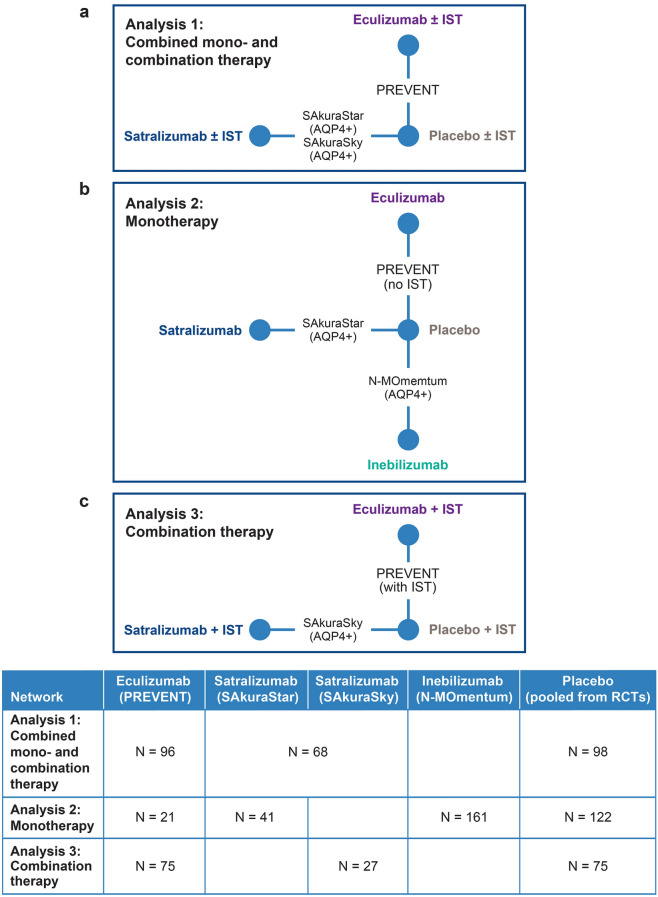
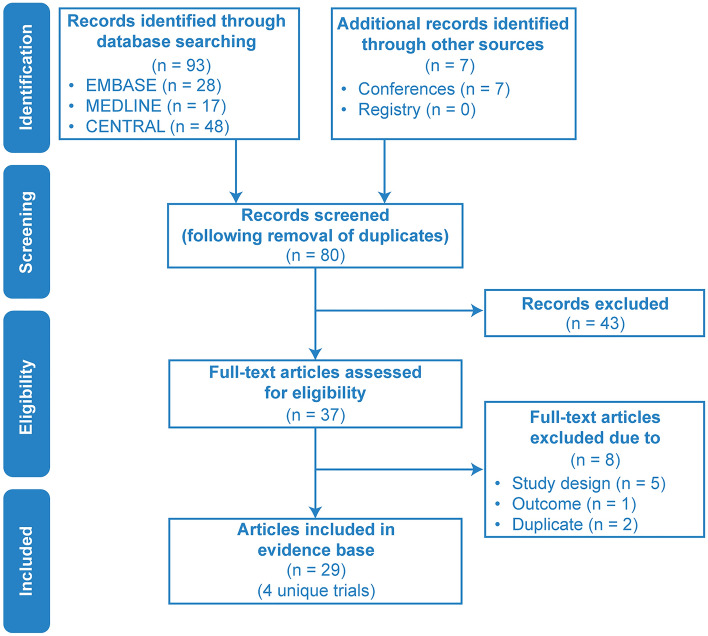
A network meta-analysis (NMA) of all U.S. Food and Drug Administration-approved therapies (eculizumab, inebilizumab, and satralizumab) for adults with aquaporin-4 immunoglobulin G-positive (AQP4+) NMOSD was conducted via a systematic literature review (SLR) using data from randomized controlled trials (RCTs). Database searches of MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials were executed for the SLR. A fixed-effects proportional hazards Bayesian NMA was used to estimate relative treatment effects based on data extracted from RCTs identified during the SLR (search end date: 11 September 2020). Four unique RCTs (N-MOmentum, PREVENT, SAkuraSky, and SAkuraStar) were identified, and data from 29 publications were extracted for analysis. Network scenarios describing the most comparable patient population groups (such as by treatment settings) were evaluated in our analyses. Relative treatment effects were evaluated based on time-to-first relapse and were expressed as hazard ratios (HRs) with 95% credible intervals (CrIs).
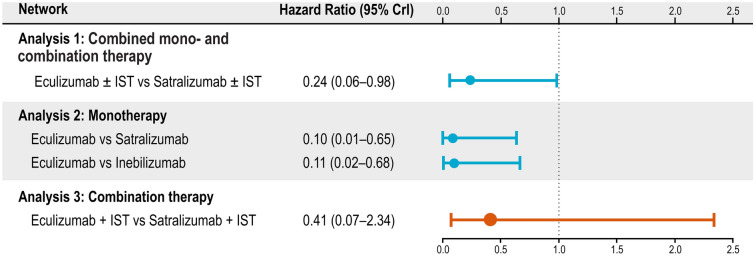
In patients treated with a monoclonal antibody only, eculizumab was associated with a lower risk of relapse compared with satralizumab (HR 0.10, 95% CrI 0.01, 0.65) and inebilizumab (HR 0.11, 95% CrI 0.02, 0.68). In patients treated with monoclonal antibody with or without background immunosuppressive therapy (IST), patients treated with eculizumab ± IST were also less likely to relapse than patients treated with satralizumab ± IST (HR 0.24, 95% CrI 0.06, 0.98).
The NMA results suggest that complement component 5 (C5) inhibition prevents NMOSD relapses more effectively than broader mechanisms of action.
视神经脊髓炎谱系障碍(NMOSD)是一种自身免疫性疾病,其特征是中枢神经系统受到攻击,导致不可逆转的损害。NMOSD治疗方法最近获得批准,因此有必要对其疗效进行比较研究,以为治疗决策提供参考。
通过系统文献综述(SLR),利用随机对照试验(RCT)的数据,对美国食品药品监督管理局批准的所有用于水通道蛋白4免疫球蛋白G阳性(AQP4+)成人NMOSD的疗法(依库珠单抗、inebilizumab和萨特利珠单抗)进行网络荟萃分析(NMA)。为进行SLR,对MEDLINE、EMBASE和Cochrane对照试验中央注册库进行了数据库检索。采用固定效应比例风险贝叶斯NMA,根据从SLR期间确定的RCT中提取的数据估计相对治疗效果(检索截止日期:2020年9月11日)。确定了四项独特的RCT(N-MOmentum、PREVENT、SAkuraSky和SAkuraStar),并提取了29篇出版物的数据进行分析。在我们的分析中评估了描述最具可比性患者群体的网络情景(如按治疗设置)。根据首次复发时间评估相对治疗效果,并以风险比(HRs)和95%可信区间(CrIs)表示。
在仅接受单克隆抗体治疗的患者中,与萨特利珠单抗(HR 0.10,95% CrI 0.01,0.65)和inebilizumab(HR 0.11,95% CrI 0.02,0.68)相比,依库珠单抗与较低的复发风险相关。在接受单克隆抗体治疗且有或无背景免疫抑制治疗(IST)的患者中,接受依库珠单抗±IST治疗的患者也比接受萨特利珠单抗±IST治疗的患者复发可能性更低(HR 0.24,95% CrI 0.06,0.98)。
NMA结果表明,补体成分5(C5)抑制比更广泛的作用机制更有效地预防NMOSD复发。