Department of Surgical Oncology, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Thoracic/Head and Neck Medical Oncology, University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Oncoimmunology. 2021 Nov 6;10(1):1992880. doi: 10.1080/2162402X.2021.1992880. eCollection 2021.
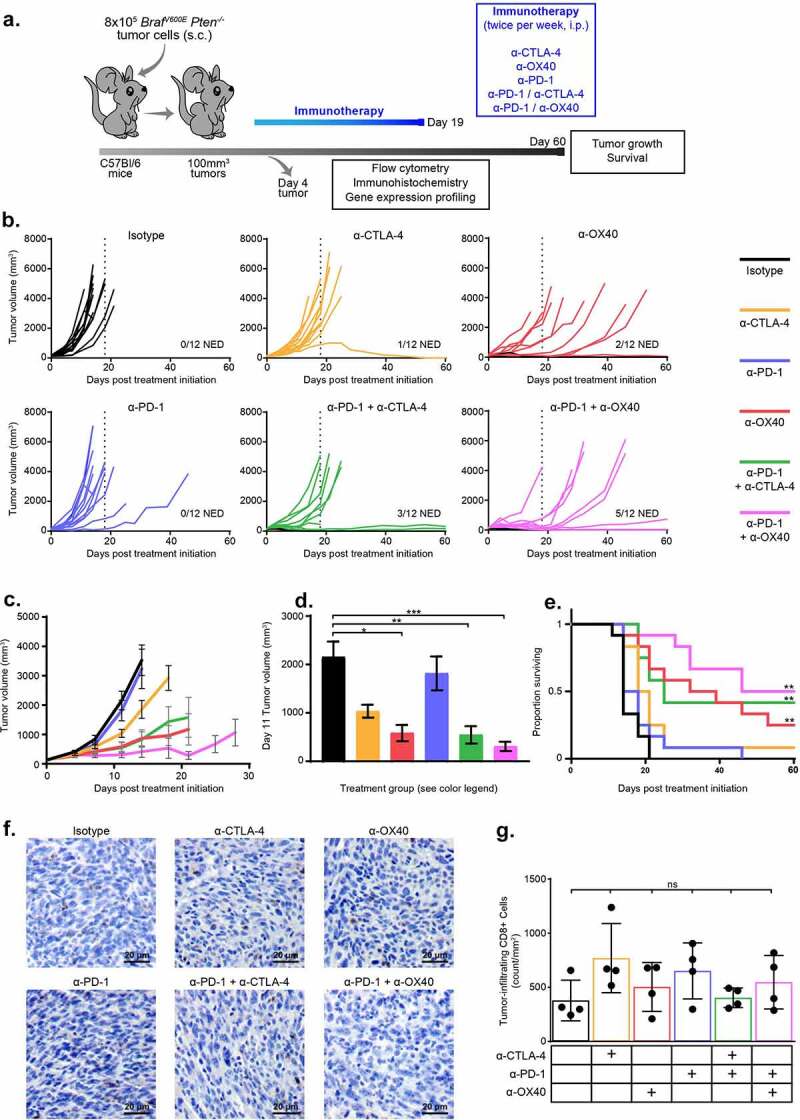
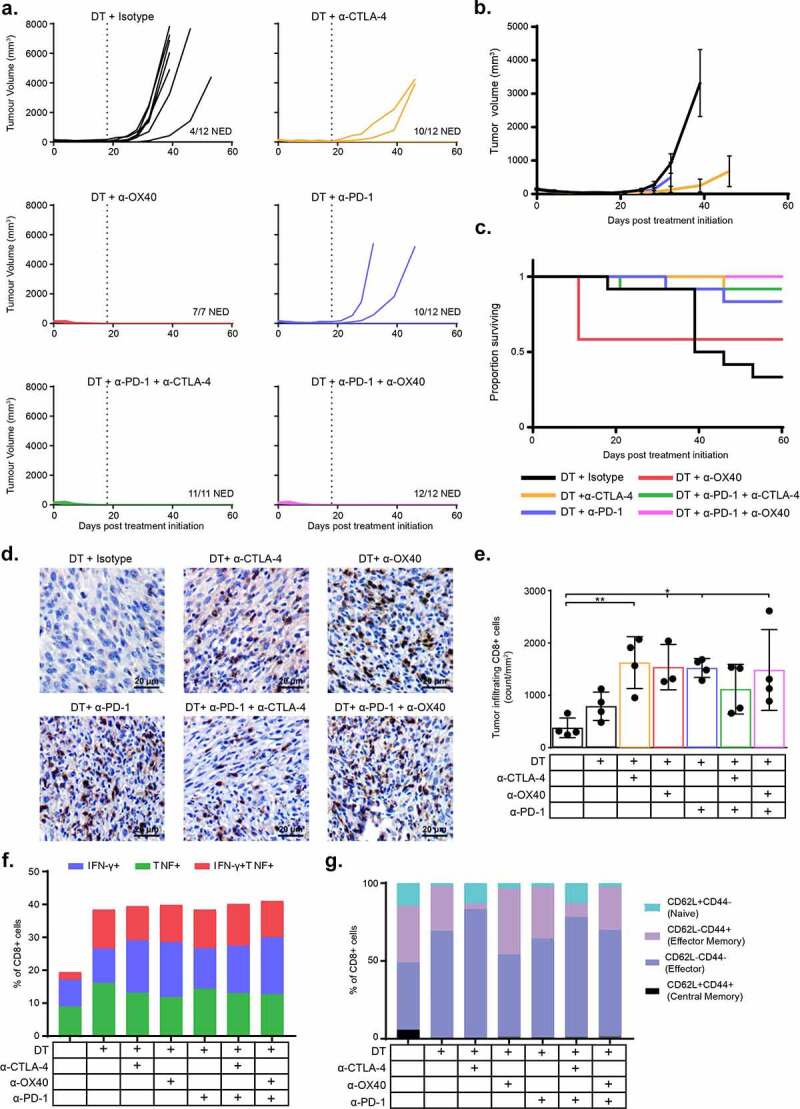
Targeted and immunotherapy regimens have revolutionized the treatment of advanced melanoma patients. Despite this, only a subset of patients respond durably. Recently, combination strategies of BRAF/MEK inhibitors with immune checkpoint inhibitor monotherapy (α-CTLA-4 or α-PD-1) have increased the rate of durable responses. Based on evidence from our group and others, these therapies appear synergistic, but at the cost of significant toxicity. We know from other treatment paradigms (e.g. hematologic malignancies) that combination strategies with multi-drug regimens (>4 drugs) are associated with more durable disease control. To better understand the mechanism of these improved outcomes, and to identify and prioritize new strategies for testing, we studied several multi-drug regimens combining BRAF/MEK targeted therapy and immunotherapy combinations in a -mutant murine melanoma model ( ). Short-term treatment with α-PD-1 and α-CTLA-4 monotherapies were relatively ineffective, while treatment with α-OX40 demonstrated some efficacy [17% of mice with no evidence of disease, (NED), at 60-days]. Outcomes were improved in the combined α-OX40/α-PD-1 group (42% NED). Short-term treatment with quadruplet therapy of immunotherapy doublets in combination with targeted therapy [dabrafenib and trametinib (DT)] was associated with excellent tumor control, with 100% of mice having NED after combined DT/α-CTLA-4/α-PD-1 or DT/α-OX40/α-PD-1. Notably, tumors from mice in these groups demonstrated a high proportion of effector memory T cells, and immunologic memory was maintained with tumor re-challenge. Together, these data provide important evidence regarding the potential utility of multi-drug therapy in treating advanced melanoma and suggest these models can be used to guide and prioritize combinatorial treatment strategies.
靶向治疗和免疫治疗方案彻底改变了晚期黑色素瘤患者的治疗方法。尽管如此,只有一部分患者能持久缓解。最近,BRAF/MEK 抑制剂联合免疫检查点抑制剂单药(α-CTLA-4 或 α-PD-1)的联合策略提高了持久缓解率。基于我们团队和其他团队的证据,这些治疗方法似乎具有协同作用,但代价是显著的毒性。我们从其他治疗方案(例如血液恶性肿瘤)中知道,联合多种药物方案(>4 种药物)的策略与更持久的疾病控制相关。为了更好地理解这些改善结果的机制,并确定和优先考虑新的测试策略,我们在一个 -mutant 鼠黑色素瘤模型()中研究了几种联合 BRAF/MEK 靶向治疗和免疫治疗组合的多药方案。短期使用 α-PD-1 和 α-CTLA-4 单药治疗相对无效,而使用 α-OX40 治疗则显示出一定的疗效[60 天时有 17%的小鼠无疾病证据(NED)]。联合 α-OX40/α-PD-1 组的结果得到改善(42%的 NED)。联合靶向治疗(dabrafenib 和 trametinib(DT))的免疫治疗双药联合四药方案的短期治疗与出色的肿瘤控制相关,联合 DT/α-CTLA-4/α-PD-1 或 DT/α-OX40/α-PD-1 治疗的所有小鼠均无疾病(NED)。值得注意的是,来自这些组的小鼠的肿瘤表现出高比例的效应记忆 T 细胞,并且在肿瘤再挑战时保持免疫记忆。总之,这些数据为多药治疗治疗晚期黑色素瘤的潜在效用提供了重要证据,并表明这些模型可用于指导和优先考虑组合治疗策略。