Department of Neurology Stroke Research Center Fujian Medical University Union Hospital Fuzhou China.
Institute of Clinical Neurology Fujian Medical University Fuzhou China.
J Am Heart Assoc. 2021 Dec 7;10(23):e022303. doi: 10.1161/JAHA.121.022303. Epub 2021 Nov 15.
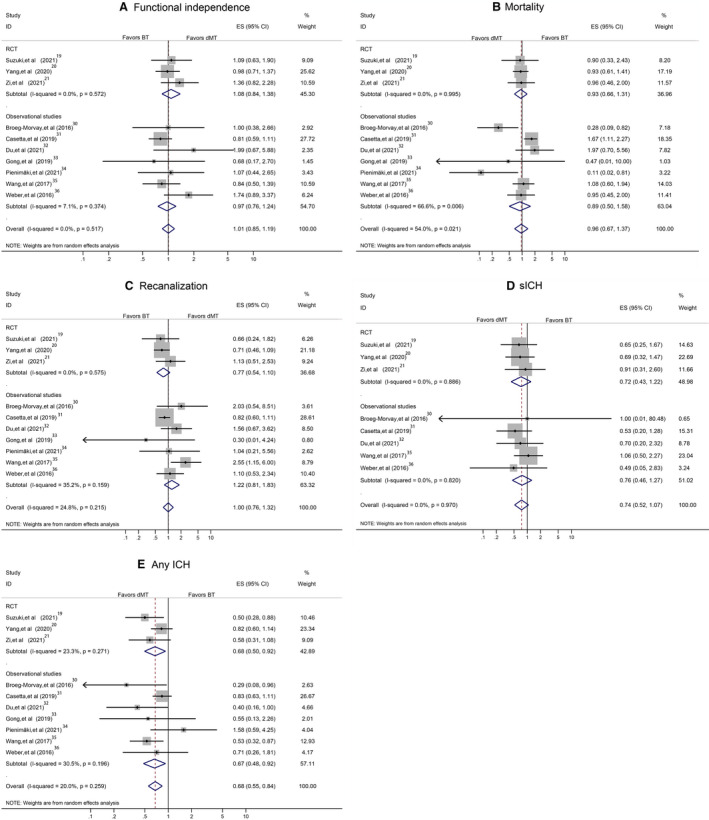
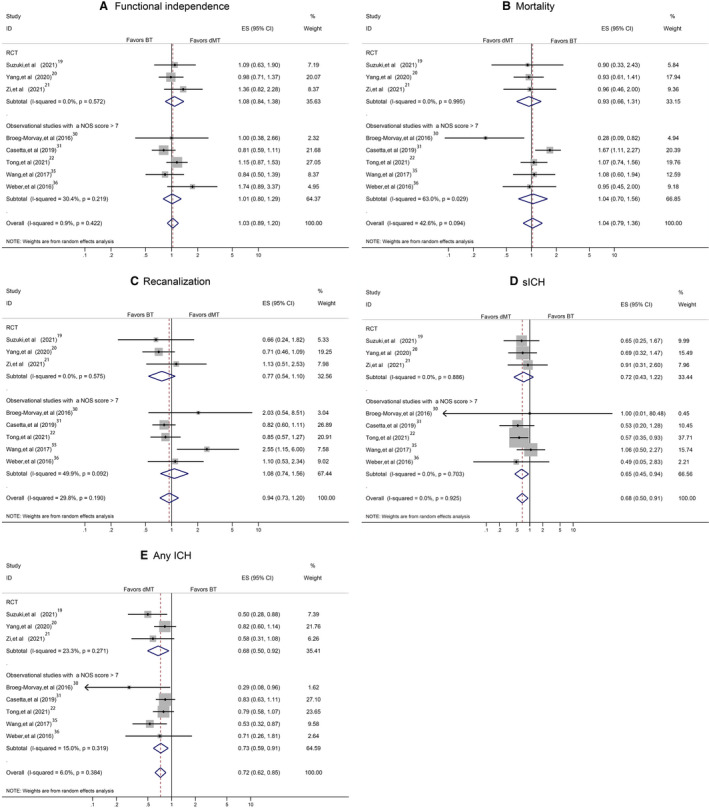
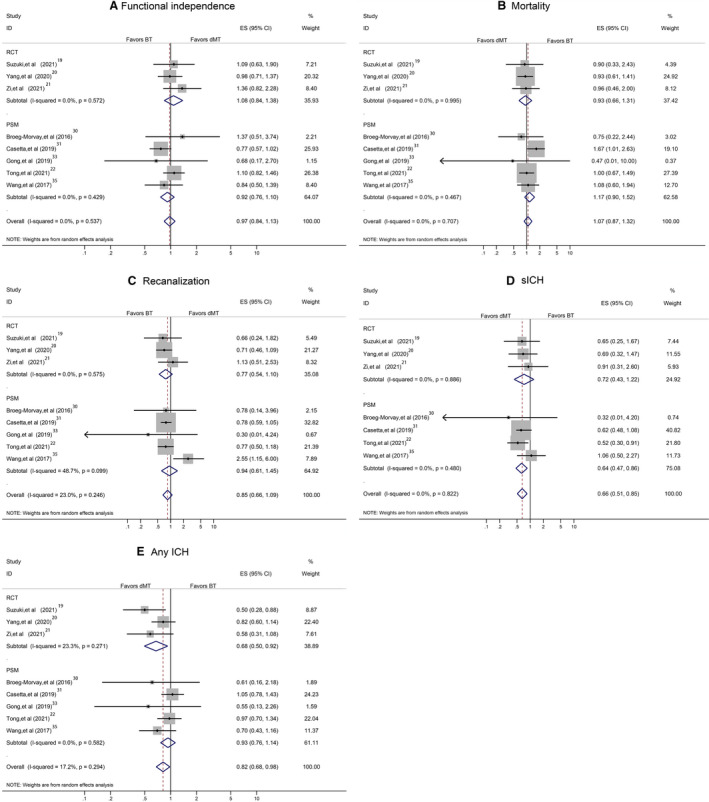
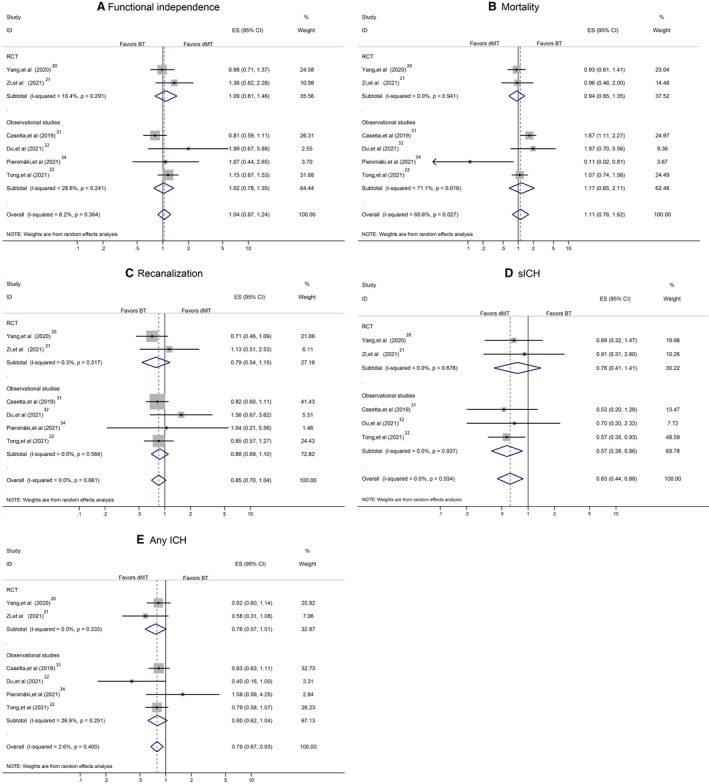
Background Whether intravenous thrombolysis before mechanical thrombectomy provides additional benefit for functional outcome in acute ischemic stroke remains uncertain. We performed a meta-analysis to compare the outcomes of direct mechanical thrombectomy (dMT) to mechanical thrombectomy with bridging using intravenous thrombolysis (bridging therapy [BT]) in patients with acute ischemic stroke. Methods and Results We performed a literature search in the PubMed, Excerpta Medica database, and Cochrane Central Register of Controlled Trials from January 1, 2003, to April 26, 2021. We included randomized clinical trials and observational studies that reported the 90-day functional outcome in patients with acute ischemic stroke undergoing dMT compared with BT. The 12 included studies (3 randomized controlled trials and 9 observational studies) yielded 3924 participants (mean age, 68.0 years [SD, 13.1 years]; women, 44.2%; 1887 participants who received dMT and 2037 participants who received BT). A meta-analysis of randomized controlled trial and observational data revealed similar 90-day functional independence (odds ratio [OR], 1.04; 95% CI, 0.90-1.19), mortality (OR, 1.03; 95% CI, 0.78-1.36), and successful recanalization (OR, 0.93; 95% CI, 0.76-1.14) for patients treated with dMT or BT. Compared with those in the BT group, patients in the dMT group were less likely to experience symptomatic intracranial hemorrhage (OR, 0.68; 95% CI, 0.51-0.91; =0.008) or any intracranial hemorrhage (OR, 0.71; 95% CI, 0.61-0.84; <0.001). Conclusions In this meta-analysis of patients with acute ischemic stroke, we found no significant differences in 90-day functional outcome or mortality between dMT and BT, but a lower rate of symptomatic intracranial hemorrhage for dMT. These findings support the use of dMT without intravenous thrombolysis bridging therapy. Registration URL: https://www.crd.york.ac.uk/prospero/; Unique identifier: 42021234664.
在急性缺血性脑卒中患者中,静脉溶栓桥接机械取栓治疗与直接机械取栓治疗相比,是否能改善功能结局仍不确定。我们进行了一项荟萃分析,以比较急性缺血性脑卒中患者接受直接机械取栓(dMT)与机械取栓桥接静脉溶栓(桥接治疗[BT])的结局。
我们在 2003 年 1 月 1 日至 2021 年 4 月 26 日期间,在 PubMed、Excerpta Medica 数据库和 Cochrane 对照试验中心注册库中进行了文献检索。我们纳入了报道急性缺血性脑卒中患者接受 dMT 与 BT 治疗后 90 天功能结局的随机临床试验和观察性研究。12 项纳入的研究(3 项随机对照试验和 9 项观察性研究)共纳入 3924 名患者(平均年龄 68.0 岁[标准差 13.1 岁];女性 44.2%;1887 名接受 dMT 治疗的患者和 2037 名接受 BT 治疗的患者)。随机对照试验和观察性数据的荟萃分析显示,接受 dMT 或 BT 治疗的患者 90 天功能独立性(比值比[OR],1.04;95%置信区间[CI],0.90-1.19)、死亡率(OR,1.03;95%CI,0.78-1.36)和成功再通率(OR,0.93;95%CI,0.76-1.14)相似。与 BT 组相比,dMT 组患者发生症状性颅内出血的可能性较小(OR,0.68;95%CI,0.51-0.91;=0.008)或任何颅内出血(OR,0.71;95%CI,0.61-0.84;<0.001)的可能性较小。
在这项急性缺血性脑卒中患者的荟萃分析中,我们发现 dMT 与 BT 治疗在 90 天功能结局或死亡率方面无显著差异,但 dMT 的症状性颅内出血发生率较低。这些发现支持在不进行静脉溶栓桥接治疗的情况下使用 dMT。