Department of Paediatrics, Division of Cardiology, The Hospital for Sick Children, University of Toronto, Labatt Family Heart Center, 555 University Avenue, Toronto, ON, M5G 1X8, Canada.
Division of Radiology and Nuclear Medicine, Pediatric section, Rikshospitalet, Oslo University Hospital, Oslo, Norway.
J Cardiovasc Magn Reson. 2021 Nov 15;23(1):134. doi: 10.1186/s12968-021-00782-9.
The extent and significance in of cardiac remodeling in Fontan patients are unclear and were the subject of this study.
This retrospective cohort study compared cardiovascular magnetic resonance (CMR) imaging markers of cardiac function, myocardial fibrosis, and hemodynamics in young Fontan patients to controls.
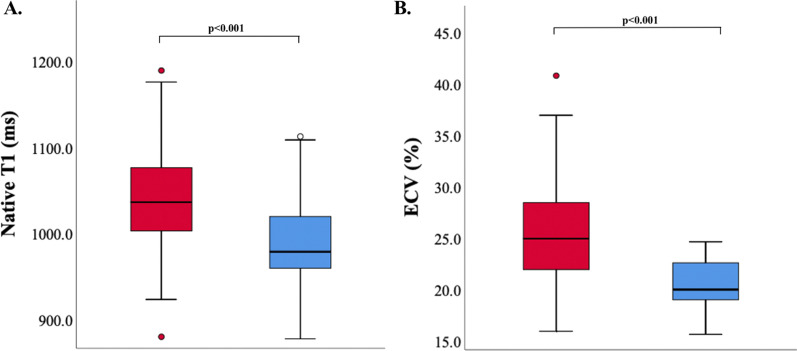
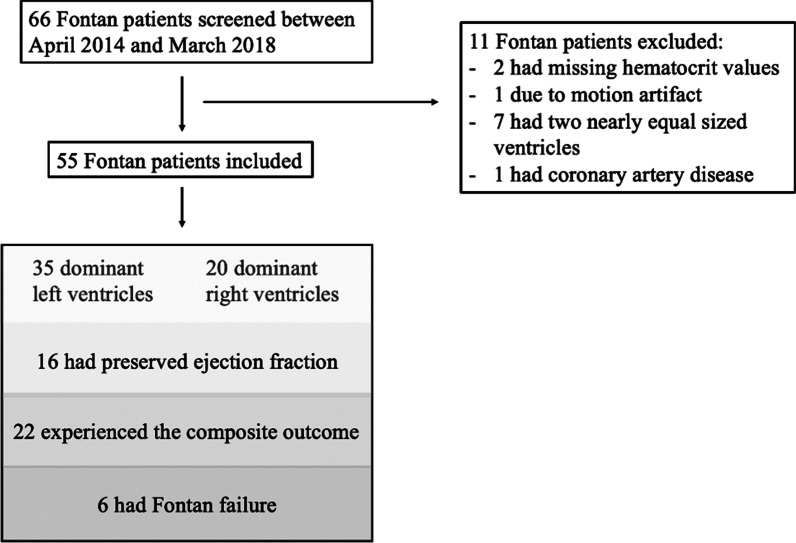
Fifty-five Fontan patients and 44 healthy controls were included (median age 14 years (range 7-17 years) vs 13 years (range 4-14 years), p = 0.057). Fontan patients had a higher indexed end-diastolic ventricular volume (EDVI 129 ml/m vs 93 ml/m, p < 0.001), and lower ejection fraction (EF 45% vs 58%, p < 0.001), circumferential (CS - 23.5% vs - 30.8%, p < 0.001), radial (6.4% vs 8.2%, p < 0.001), and longitudinal strain (- 13.3% vs - 24.8%, p < 0.001). Compared to healthy controls, Fontan patients had higher extracellular volume fraction (ECV) (26.3% vs 20.6%, p < 0.001) and native T1 (1041 ms vs 986 ms, p < 0.001). Patients with a dominant right ventricle demonstrated larger ventricles (EDVI 146 ml/m vs 120 ml/m, p = 0.03), lower EF (41% vs 47%, p = 0.008), worse CS (- 20.1% vs - 25.6%, p = 0.003), and a trend towards higher ECV (28.3% versus 24.1%, p = 0.09). Worse EF and CS correlated with longer cumulative bypass (R = - 0.36, p = 0.003 and R = 0.46, p < 0.001), cross-clamp (R = - 0.41, p = 0.001 and R = 0.40, p = 0.003) and circulatory arrest times (R = - 0.42, p < 0.001 and R = 0.27, p = 0.03). T1 correlated with aortopulmonary collateral (APC) flow (R = 0.36, p = 0.009) which, in the linear regression model, was independent of ventricular morphology (p = 0.9) and EDVI (p = 0.2). The composite outcome (cardiac readmission, cardiac reintervention, Fontan failure or any clinically significant arrhythmia) was associated with increased native T1 (1063 ms vs 1026 ms, p = 0.029) and EDVI (146 ml/m vs 118 ml/m, p = 0.013), as well as decreased EF (42% vs 46%, p = 0.045) and worse CS (- 22% vs - 25%, p = 0.029). APC flow (HR 5.5 CI 1.9-16.2, p = 0.002) was independently associated with the composite outcome, independent of ventricular morphology (HR 0.71 CI 0.30-1.69 p = 0.44) and T1 (HR1.006 CI 1.0-1.13, p = 0.07).
Pediatric Fontan patients have ventricular dysfunction, altered myocardial mechanics and increased fibrotic remodeling. Cumulative exposure to cardiopulmonary bypass and increased aortopulmonary collateral flow are associated with myocardial dysfunction and fibrosis. Cardiac dysfunction, fibrosis, and collateral flow are associated with adverse outcomes.
心腔重构在 Fontan 患者中的程度和意义尚不清楚,这是本研究的主题。
本回顾性队列研究比较了心血管磁共振(CMR)成像在心脏功能、心肌纤维化和血流动力学方面的标志物,以评估 Fontan 患者与对照组的差异。
共纳入 55 例 Fontan 患者和 44 名健康对照者(中位年龄 14 岁[范围 7-17 岁]与 13 岁[范围 4-14 岁],p=0.057)。Fontan 患者的左室舒张末期容积指数(EDVI)更高(129ml/m2 与 93ml/m2,p<0.001),射血分数(EF)更低(45% 与 58%,p<0.001),周向应变(CS)更低(-23.5% 与 -30.8%,p<0.001),径向应变(6.4% 与 8.2%,p<0.001),纵向应变(-13.3% 与 -24.8%,p<0.001)。与健康对照组相比,Fontan 患者的细胞外容积分数(ECV)更高(26.3% 与 20.6%,p<0.001),心脏 T1 值(1041ms 与 986ms,p<0.001)更长。右心室优势的患者心室更大(EDVI 146ml/m2 与 120ml/m2,p=0.03),EF 更低(41% 与 47%,p=0.008),CS 更差(-20.1% 与 -25.6%,p=0.003),ECV 呈升高趋势(28.3% 与 24.1%,p=0.09)。EF 和 CS 越差与更长的体外循环(R=-0.36,p=0.003 和 R=-0.46,p<0.001)、体外循环夹闭(R=-0.41,p=0.001 和 R=-0.40,p=0.003)和停循环时间(R=-0.42,p<0.001 和 R=-0.27,p=0.03)相关。T1 值与体肺侧支循环(APC)血流量相关(R=0.36,p=0.009),在线性回归模型中,T1 值与心室形态(p=0.9)和 EDVI(p=0.2)无关。复合终点(心脏再入院、心脏再介入、Fontan 衰竭或任何有临床意义的心律失常)与升高的 T1 值(1063ms 与 1026ms,p=0.029)和 EDVI(146ml/m2 与 118ml/m2,p=0.013),以及降低的 EF(42% 与 46%,p=0.045)和更差的 CS(-22% 与 -25%,p=0.029)相关。APC 血流量(HR 5.5,95%CI 1.9-16.2,p=0.002)与复合终点独立相关,与心室形态(HR 0.71,95%CI 0.30-1.69,p=0.44)和 T1(HR 1.006,95%CI 1.0-1.13,p=0.07)无关。
儿科 Fontan 患者存在心室功能障碍、心肌力学改变和纤维化重构增加。体外循环和体肺侧支循环血流量的累积暴露与心肌功能障碍和纤维化相关。心功能障碍、纤维化和侧支循环与不良结局相关。