Department of Cardiology, Boston Children's Hospital, 300 Longwood Ave, Boston, MA, 02115, USA.
Department of Pediatrics, Harvard Medical School, Boston, MA, USA.
J Cardiovasc Magn Reson. 2022 Nov 14;24(1):56. doi: 10.1186/s12968-022-00884-y.
Cross-sectional studies have reported that ventricular dilation and dysfunction are associated with adverse clinical outcome in Fontan patients; however, longitudinal changes and their relationship with outcome are not known.
This was a single-center retrospective analysis of Fontan patients with at least 2 cardiovascular magnetic resonance (CMR) scans without intervening interventions. Serial measures of end-diastolic volume index (EDVI), end-systolic volume index (ESVI), ejection fraction (EF), indexed mass (mass), mass-to-volume ratio, and end-systolic wall stress (ESWS) were used to estimate within-patient change over time. Changes were compared for those with and without a composite outcome (death, heart transplant, or transplant listing) as well as between patients with left (LV) and right ventricular (RV) dominance.
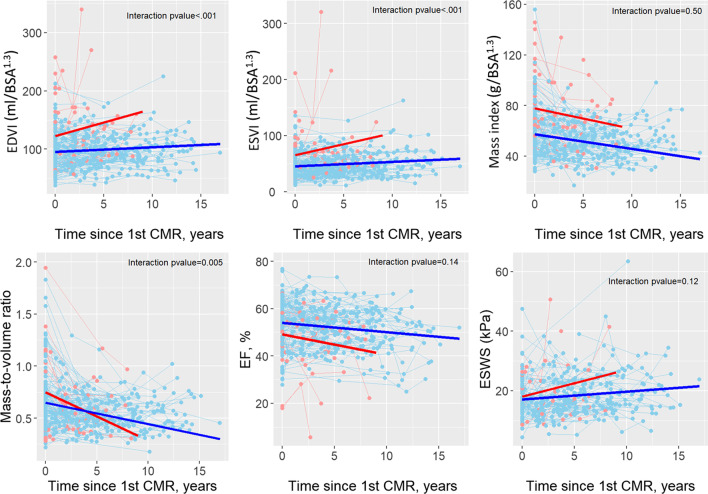
Data from 156 patients were analyzed with a mean age at 1st CMR of 17.8 ± 9.6 years. 490 CMRs were included with median of 3 CMRs/patient (range 2-9). On regression analysis with mixed effects models, volumes and ESWS increased, while mass, mass-to-volume ratio, and EF decreased over time. With a median follow-up of 10.2 years, 14% met the composite outcome. Those with the composite outcome had a greater increase in EDVI compared to those without (4.7 vs. 0.8 ml/BSA/year). Compared with LV dominance, RV dominance was associated with a greater increase in ESVI (1.4 vs. 0.5 ml/BSA/year), a greater decrease in EF (- 0.61%/year vs. - 0.24%/year), and a higher rate of the composite outcome (21% vs. 8%).
Ventricles in the Fontan circulation exhibit a steady decline in performance with an increase in EDVI, ESVI, and ESWS, and decrease in EF, mass index, and mass-to-volume ratio. Those with death or need for heart transplantation have a faster increase in EDVI. Patients with rapid increase in EDVI (> 5 ml/BSA/year) may be at a higher risk of adverse outcomes and may benefit from closer surveillance. RV dominance is associated with worse clinical outcomes and remodeling compared to LV dominance.
横断面研究报告称,在 Fontan 患者中,心室扩张和功能障碍与不良临床结局相关;然而,纵向变化及其与结局的关系尚不清楚。
这是一项单中心回顾性分析,纳入了至少有 2 次心血管磁共振(CMR)扫描且无介入干预的 Fontan 患者。使用舒张末期容积指数(EDVI)、收缩末期容积指数(ESVI)、射血分数(EF)、指数化质量(mass)、质量与容积比和收缩末期壁应力(ESWS)的系列测量值来估计患者个体随时间的变化。比较了有和无复合结局(死亡、心脏移植或移植名单)以及左心室(LV)和右心室(RV)优势患者之间的变化。
对 156 名患者的数据进行了分析,首次 CMR 的平均年龄为 17.8±9.6 岁。纳入了 490 次 CMR,中位数为 3 次/患者(范围 2-9)。在混合效应模型的回归分析中,体积和 ESWS 随时间增加,而质量、质量与容积比和 EF 随时间减少。中位随访 10.2 年后,14%的患者发生了复合结局。与无复合结局的患者相比,发生复合结局的患者 EDVI 增加更多(4.7 比 0.8 ml/BSA/年)。与 LV 优势相比,RV 优势与 ESVI 增加更多(1.4 比 0.5 ml/BSA/年)、EF 下降更多(-0.61%/年比-0.24%/年)和复合结局发生率更高(21%比 8%)有关。
Fontan 循环中的心室表现出性能逐渐下降,EDVI、ESVI 和 ESWS 增加,EF、质量指数和质量与容积比降低。EDVI 增加更快的患者死亡或需要心脏移植的风险更高。EDVI 增加超过 5 ml/BSA/年的患者可能有更高的不良结局风险,可能需要更密切的监测。与 LV 优势相比,RV 优势与更差的临床结局和重构相关。