Department of Surgery, Campus Charité Mitte and Campus Virchow-Klinikum, Charité Universitätsmedizin Berlin, Augustenburger Platz 1, 13353, Berlin, Germany.
Berlin Institute of Health, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117, Berlin, Germany.
Langenbecks Arch Surg. 2022 Feb;407(1):235-244. doi: 10.1007/s00423-021-02361-z. Epub 2021 Nov 17.
The aim of this study was to analyze the impact of minimally invasive intermittent Pringle maneuver (IPM) on postoperative outcomes in patients with hepatocellular carcinoma (HCC) and liver cirrhosis.
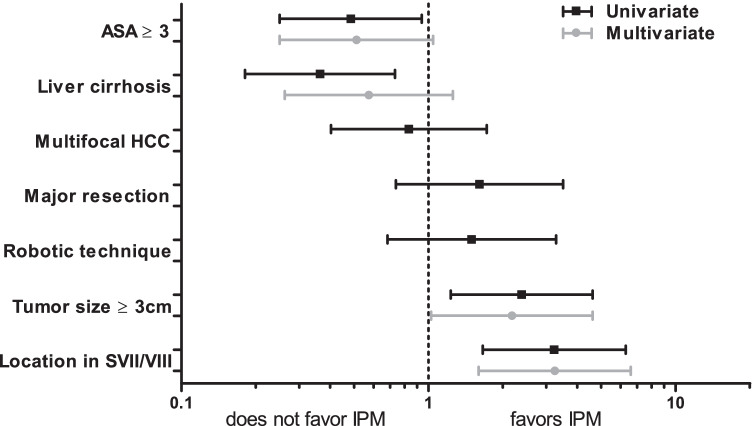
In this retrospective cohort study, we evaluated the safety of IPM in patients with HCC who underwent minimally invasive liver resection during five years at our center. Factors influencing the use of IPM were examined in univariate and multivariate regression analysis. Cases with use of IPM (IPM) and those without use of IPM (no IPM) were then compared regarding intraoperative and postoperative outcomes after propensity score matching (PSM) for surgical difficulty.
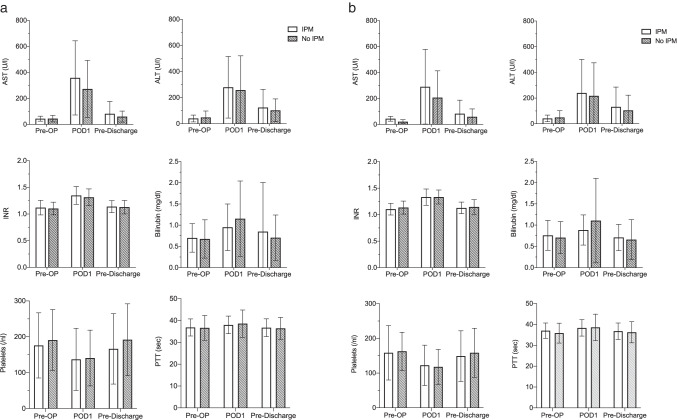
One hundred fifty-one patients underwent liver resection for HCC at our center and met inclusion criteria. Of these, 73 patients (48%) received IPM with a median duration of 18 min (5-78). One hundred patients (66%) had confirmed liver cirrhosis. In multivariate analysis, patients with large tumors (≥ 3 cm) and difficult tumor locations (segments VII or VIII) were more likely to undergo IPM (OR 1.176, p = 0.043, and OR 3.243, p = 0.001, respectively). After PSM, there were no differences in intraoperative blood transfusion or postoperative complication rates between the IPM and no IPM groups. Neither did we observe any differences in the subgroup analysis for cirrhotic patients. Postoperative serum liver function tests were not affected by the use of IPM.
Based on our findings, we conclude that the use of IPM in minimally invasive liver resection is safe and feasible for patients with HCC, including those with compensated liver cirrhosis.
本研究旨在分析微创间歇性阻断入肝血流(IPM)对伴有肝硬化的肝细胞癌(HCC)患者术后结局的影响。
在这项回顾性队列研究中,我们评估了 5 年内我院接受微创肝切除术的 HCC 患者使用 IPM 的安全性。在单变量和多变量回归分析中检查了影响 IPM 使用的因素。在倾向评分匹配(PSM)以调整手术难度后,比较了使用 IPM(IPM 组)和未使用 IPM(无 IPM 组)患者的术中及术后结局。
我院共有 151 例 HCC 患者符合纳入标准并接受了肝切除术。其中 73 例(48%)患者采用了 IPM,其阻断时间中位数为 18 分钟(5-78 分钟)。100 例(66%)患者合并肝硬化。多变量分析显示,肿瘤较大(≥3cm)和肿瘤位置困难(VII 或 VIII 段)的患者更可能采用 IPM(OR 1.176,p=0.043,OR 3.243,p=0.001)。PSM 后,IPM 组与无 IPM 组之间的术中输血或术后并发症发生率无差异。对肝硬化患者的亚组分析也未见差异。IPM 的使用并未影响术后肝功能检查结果。
根据我们的发现,我们得出结论,微创肝切除术中使用 IPM 对 HCC 患者(包括代偿期肝硬化患者)是安全且可行的。