Department of Surgery, Leiden University Medical Centre, Leiden, the Netherlands.
Department of Surgery, Cancer Centre Amsterdam, Amsterdam UMC, University of Amsterdam, Amsterdam, the Netherlands.
Br J Surg. 2021 Dec 17;109(1):96-104. doi: 10.1093/bjs/znab345.
Venous resection of the superior mesenteric or portal vein is increasingly performed in pancreatic cancer surgery, whereas results of studies on short- and long-term outcomes are contradictory. The aim of this study was to evaluate the impact of the type of venous resection in pancreatoduodenectomy for pancreatic cancer on postoperative morbidity and overall survival.
This nationwide retrospective cohort study included all patients who underwent pancreatoduodenectomy for pancreatic cancer in 18 centres (2013-2017).
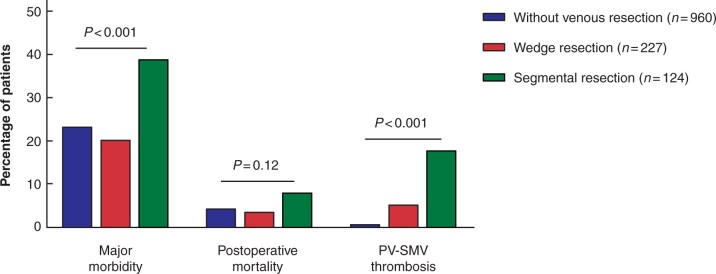
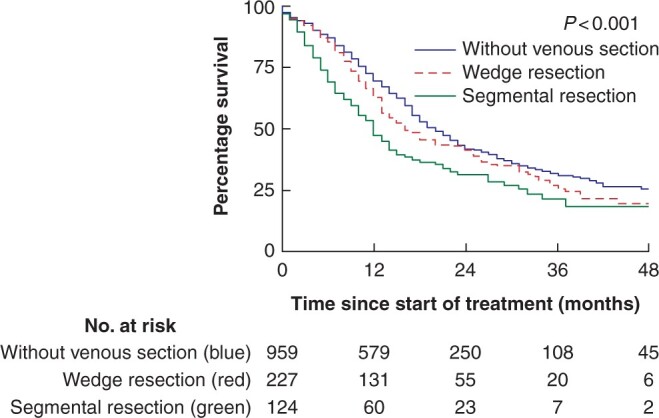
A total of 1311 patients were included, of whom 17 per cent underwent wedge resection and 10 per cent segmental resection. Patients with segmental resection had higher rates of major morbidity (39 versus 20 versus 23 per cent, respectively; P < 0.001) and portal or superior mesenteric vein thrombosis (18 versus 5 versus 1 per cent, respectively; P < 0.001) and worse overall survival (median 12 versus 16 versus 20 months, respectively; P < 0.001), compared to patients with wedge resection and those without venous resection. Multivariable analysis showed patients with segmental resection, but not those who had wedge resection, had higher rates of major morbidity (odds ratio = 1.93, 95 per cent c.i. 1.20 to 3.11) and worse overall survival (hazard ratio = 1.40, 95 per cent c.i. 1.10 to 1.78), compared to patients without venous resection. Among patients who received neoadjuvant therapy, there was no difference in overall survival among patients with segmental and wedge resection and those without venous resection (median 32 versus 25 versus 33 months, respectively; P = 0.470), although there was a difference in major morbidity rates (52 versus 19 versus 21 per cent, respectively; P = 0.012).
In pancreatic surgery, the short- and long-term outcomes are worse in patients with venous segmental resection, compared to patients with wedge resection and those without venous resection.
在胰腺癌手术中,越来越多地进行肠系膜上静脉或门静脉切除术,然而关于短期和长期结果的研究结果却存在矛盾。本研究旨在评估在胰十二指肠切除术治疗胰腺癌中静脉切除术类型对术后发病率和总体生存率的影响。
这是一项全国性回顾性队列研究,纳入了 2013 年至 2017 年期间在 18 个中心接受胰十二指肠切除术治疗胰腺癌的所有患者。
共纳入 1311 例患者,其中 17%接受楔形切除术,10%接受节段切除术。节段切除术患者的主要发病率(分别为 39%、20%和 23%,P<0.001)和门静脉或肠系膜上静脉血栓形成(分别为 18%、5%和 1%,P<0.001)以及总体生存率(分别为 12 个月、16 个月和 20 个月,P<0.001)均高于楔形切除术患者和无静脉切除术患者。多变量分析显示,与楔形切除术患者和无静脉切除术患者相比,节段切除术患者的主要发病率(比值比=1.93,95%置信区间 1.20 至 3.11)和总体生存率(风险比=1.40,95%置信区间 1.10 至 1.78)更差。在接受新辅助治疗的患者中,节段性和楔形切除术患者与无静脉切除术患者的总体生存率无差异(分别为 32 个月、25 个月和 33 个月,P=0.470),尽管主要发病率(分别为 52%、19%和 21%,P=0.012)存在差异。
在胰腺手术中,与楔形切除术患者和无静脉切除术患者相比,节段性静脉切除术患者的短期和长期结果更差。