Chae Yoon Soo, Jung Hye-Sol, Yun Won-Gun, Han Youngmin, Cho Young Jae, Lee Mirang, Kwon Wooil, Park Joon Seong, Jang Jin-Young
Department of Surgery and Cancer Research Institute, Seoul National University College of Medicine, Seoul, South Korea.
Department of Surgery, Asan Medical Center, Seoul, South Korea.
Int J Surg. 2024 Nov 1;110(11):7150-7158. doi: 10.1097/JS9.0000000000002034.
R0 rates have increased as neoadjuvant treatment (NAT) has become the primary treatment for pancreatic ductal adenocarcinoma (PDAC) with venous involvement, suggesting a decrease in venous tumor infiltration. The aim of this study was to investigate the clinical outcomes of preserving the portal/superior mesenteric vein (PV/SMV) during pancreaticoduodenectomy (PD) in PDAC patients who underwent NAT.
The 113 patients with resectable and borderline resectable PDAC with venous involvement who responded to NAT and underwent curative PD between 2012 and 2022 were retrospectively reviewed.
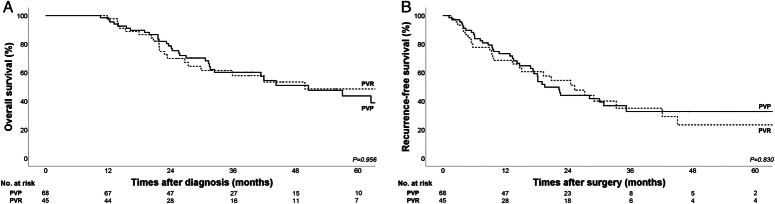
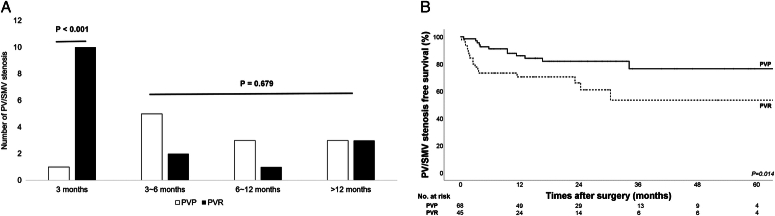
Among the 113 patients, PV/SMV preservation (PVP) was performed in 68 patients (60.2%), and PV/SMV resection (PVR) was performed in 45 patients (39.8%). There was no significant difference in the R0 rate, 5-year overall survival (OS) and recurrence-free survival between the two groups. PV/SMV stenosis within 3 months after surgery was more common in the PVR group than in the PVP group (1.5% versus 22.2%; P <0.001), and 5-year PV/SMV stenosis-free survival was significantly higher in the PVP group than in the PVR group (76.5% versus 53.4%; P =0.014). Multivariate analysis showed that gemcitabine-based neoadjuvant chemotherapy was associated with poor OS. PVR, clinically relevant postoperative pancreatic fistula, and locoregional recurrence were independent risk factors for PV/SMV stenosis.
The PVP group had similar oncologic outcomes and better vessel-functional outcomes than the PVR group. Therefore, if dissection is possible and there is a high likelihood of achieving R0 resection after NAT, routine PVR may be unnecessary in PDAC patients with venous involvement.
随着新辅助治疗(NAT)成为伴有静脉侵犯的胰腺导管腺癌(PDAC)的主要治疗方法,R0切除率有所提高,这表明静脉肿瘤浸润有所减少。本研究的目的是调查接受NAT的PDAC患者在胰十二指肠切除术(PD)期间保留门静脉/肠系膜上静脉(PV/SMV)的临床结局。
回顾性分析了2012年至2022年间113例对NAT有反应且接受了根治性PD的可切除和临界可切除的伴有静脉侵犯的PDAC患者。
113例患者中,68例(60.2%)进行了PV/SMV保留(PVP),45例(39.8%)进行了PV/SMV切除(PVR)。两组的R0切除率、5年总生存率(OS)和无复发生存率无显著差异。术后3个月内PV/SMV狭窄在PVR组比PVP组更常见(1.5%对22.2%;P<0.001),PVP组的5年无PV/SMV狭窄生存率显著高于PVR组(76.5%对53.4%;P=0.014)。多因素分析显示,基于吉西他滨的新辅助化疗与较差的OS相关。PVR、临床相关的术后胰瘘和局部区域复发是PV/SMV狭窄的独立危险因素。
与PVR组相比,PVP组具有相似的肿瘤学结局和更好的血管功能结局。因此,如果可以进行解剖且在NAT后实现R0切除的可能性很高,对于伴有静脉侵犯的PDAC患者,常规PVR可能不必要。