Department of Emergency Medicine, Atrium Health's Carolinas Medical Center, Charlotte, NC, United States of America.
Department of Emergency Medicine, Kaiser Permanente, San Diego, CA, United States of America.
PLoS One. 2021 Nov 18;16(11):e0260036. doi: 10.1371/journal.pone.0260036. eCollection 2021.
Develop and validate a prognostic model for clinical deterioration or death within days of pulmonary embolism (PE) diagnosis using point-of-care criteria.
We used prospective registry data from six emergency departments. The primary composite outcome was death or deterioration (respiratory failure, cardiac arrest, new dysrhythmia, sustained hypotension, and rescue reperfusion intervention) within 5 days. Candidate predictors included laboratory and imaging right ventricle (RV) assessments. The prognostic model was developed from 935 PE patients. Univariable analysis of 138 candidate variables was followed by penalized and standard logistic regression on 26 retained variables, and then tested with a validation database (N = 801).
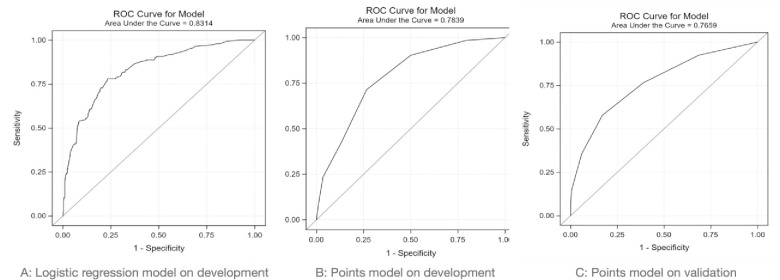
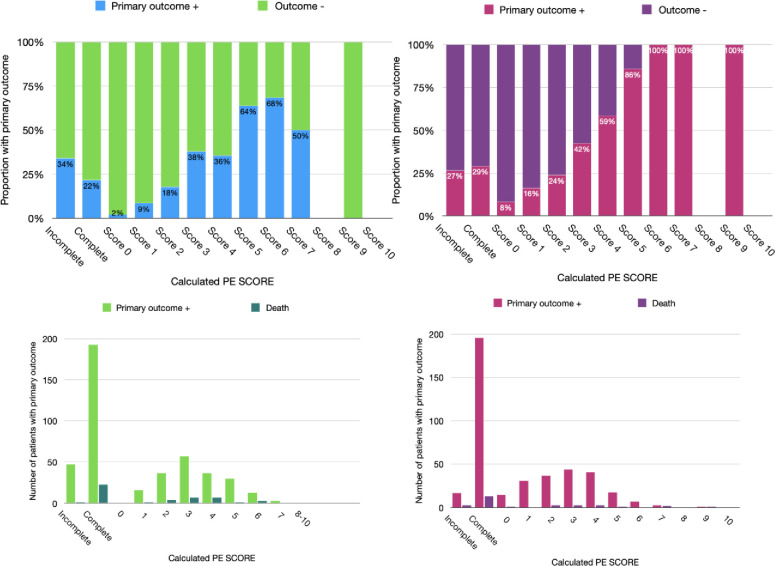
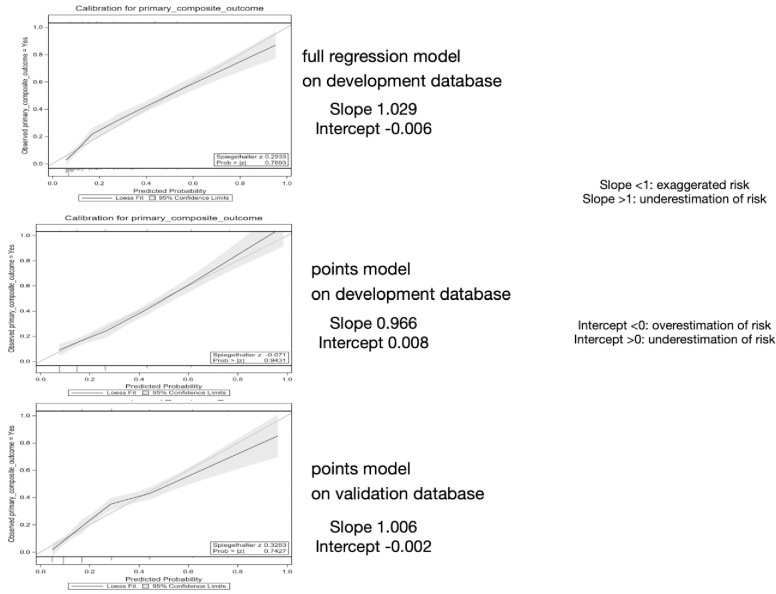
Logistic regression yielded a nine-variable model, then simplified to a nine-point tool (PE-SCORE): one point each for abnormal RV by echocardiography, abnormal RV by computed tomography, systolic blood pressure < 100 mmHg, dysrhythmia, suspected/confirmed systemic infection, syncope, medico-social admission reason, abnormal heart rate, and two points for creatinine greater than 2.0 mg/dL. In the development database, 22.4% had the primary outcome. Prognostic accuracy of logistic regression model versus PE-SCORE model: 0.83 (0.80, 0.86) vs. 0.78 (0.75, 0.82) using area under the curve (AUC) and 0.61 (0.57, 0.64) vs. 0.50 (0.39, 0.60) using precision-recall curve (AUCpr). In the validation database, 26.6% had the primary outcome. PE-SCORE had AUC 0.77 (0.73, 0.81) and AUCpr 0.63 (0.43, 0.81). As points increased, outcome proportions increased: a score of zero had 2% outcome, whereas scores of six and above had ≥ 69.6% outcomes. In the validation dataset, PE-SCORE zero had 8% outcome [no deaths], whereas all patients with PE-SCORE of six and above had the primary outcome.
PE-SCORE model identifies PE patients at low- and high-risk for deterioration and may help guide decisions about early outpatient management versus need for hospital-based monitoring.
使用床边标准,开发并验证一个可预测肺栓塞(PE)诊断后数天内临床恶化或死亡的预后模型。
我们使用了来自六个急诊室的前瞻性登记数据。主要复合结局为 5 天内死亡或恶化(呼吸衰竭、心脏骤停、新出现心律失常、持续性低血压和挽救性再灌注干预)。候选预测因素包括实验室和影像学右心室(RV)评估。该预后模型由 935 名 PE 患者建立。对 138 个候选变量进行单变量分析,然后对 26 个保留变量进行惩罚和标准逻辑回归,最后在验证数据库(N=801)中进行测试。
逻辑回归得出了一个 9 变量模型,然后简化为一个 9 分工具(PE-SCORE):超声心动图提示 RV 异常、CT 提示 RV 异常、收缩压<100mmHg、心律失常、疑似/确诊全身感染、晕厥、医疗社会入院原因、心率异常各计 1 分,肌酐>2.0mg/dL 计 2 分。在开发数据库中,22.4%的患者出现主要结局。逻辑回归模型与 PE-SCORE 模型的预后准确性:曲线下面积(AUC)为 0.83(0.80,0.86)与 0.78(0.75,0.82),精度-召回曲线(AUCpr)为 0.61(0.57,0.64)与 0.50(0.39,0.60)。在验证数据库中,26.6%的患者出现主要结局。PE-SCORE 的 AUC 为 0.77(0.73,0.81),AUCpr 为 0.63(0.43,0.81)。随着分数的增加,结局比例增加:得分为零的患者有 2%的结局,而得分为六分及以上的患者有≥69.6%的结局。在验证数据集,PE-SCORE 得分为零的患者有 8%的结局(无死亡),而所有 PE-SCORE 得分为六分及以上的患者均出现主要结局。
PE-SCORE 模型可识别 PE 患者的低危和高危恶化风险,有助于指导早期门诊管理与需要医院监测之间的决策。