Wetzell Bradley, McLean Julie B, Dorsch Kimberly, Moore Mark A
Global Scientific Affairs and Clinical Engagement, LifeNet Health®, 1864 Concert Drive, Virginia Beach, VA, 23453, USA.
Global Clinical Affairs, LifeNet Health®, Virginia Beach, VA, USA.
J Orthop Surg Res. 2021 Nov 18;16(1):680. doi: 10.1186/s13018-021-02829-0.
The objectives of this study were to build upon previously-reported 12-month findings by retrospectively comparing 24-month follow-up hospitalization charges and potentially-relevant readmissions in US lumbar fusion surgeries that employed either recombinant human bone morphogenetic protein-2 (rhBMP-2) or a cellular bone allograft comprised of viable lineage-committed bone cells (V-CBA) via a nationwide healthcare system database.
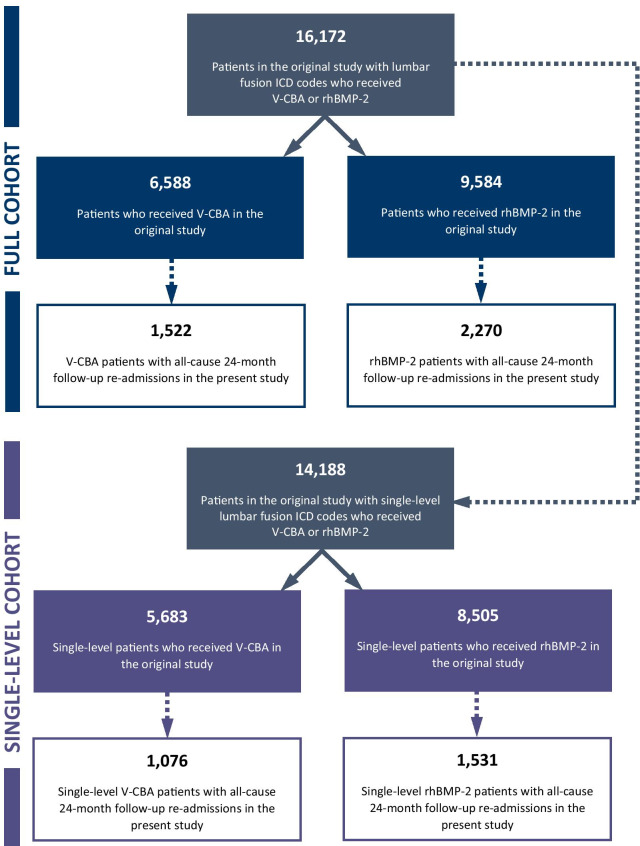
A total of 16,172 patients underwent lumbar fusion surgery using V-CBA or rhBMP-2 in the original study, of whom 3,792 patients (23.4%) were identified in the current study with all-cause readmissions during the 24-month follow-up period. Confounding baseline patient, procedure, and hospital characteristics found in the original study were used to adjust multivariate regression models comparing differences in 24-month follow-up hospitalization charges (in 2020 US dollars) and lengths of stay (LOS; in days) between the groups. Differences in potentially-relevant follow-up readmissions were also compared, and all analyses were repeated in the subset of patients who only received treatment at a single level of the spine.
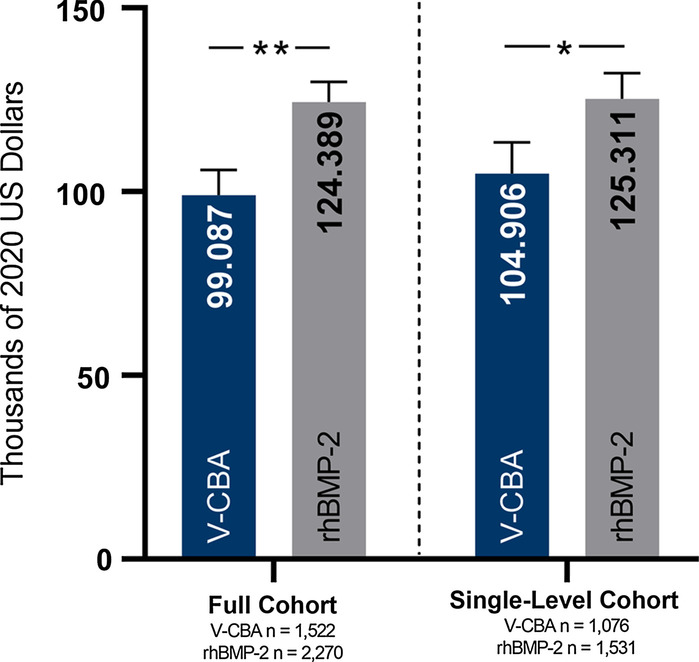
The adjusted cumulative mean 24-month follow-up hospitalization charges in the full cohort were significantly lower in the V-CBA group ($99,087) versus the rhBMP-2 group ($124,389; P < 0.0001), and this pattern remained in the single-level cohort (V-CBA = $104,906 vs rhBMP-2 = $125,311; P = 0.0006). There were no differences between groups in adjusted cumulative mean LOS in either cohort. Differences in the rates of follow-up readmissions aligned with baseline comorbidities originally reported for the initial procedure. Subsequent lumbar fusion rates were significantly lower for V-CBA patients in the full cohort (10.12% vs 12.00%; P = 0.0002) and similar between groups in the single-level cohort, in spite of V-CBA patients having significantly higher rates of baseline comorbidities that could negatively impact clinical outcomes, including bony fusion.
The results of this study suggest that use of V-CBA for lumbar fusion surgeries performed in the US is associated with substantially lower 24-month follow-up hospitalization charges versus rhBMP-2, with both exhibiting similar rates of subsequent lumbar fusion procedures and potentially-relevant readmissions.
本研究的目的是通过回顾性比较采用重组人骨形态发生蛋白-2(rhBMP-2)或由有活力的定向骨细胞组成的细胞骨移植体(V-CBA)的美国腰椎融合手术中24个月的随访住院费用及潜在相关再入院情况,以进一步分析先前报告的12个月研究结果。
在原研究中,共有16172例患者接受了使用V-CBA或rhBMP-2的腰椎融合手术,其中3792例患者(23.4%)在本研究中被确定在24个月随访期内有全因再入院情况。利用原研究中发现的患者、手术和医院的混杂基线特征来调整多变量回归模型,比较两组在24个月随访住院费用(以2020年美元计)和住院时间(LOS;以天计)方面的差异。还比较了潜在相关随访再入院的差异,并且在仅在脊柱单一节段接受治疗的患者亚组中重复了所有分析。
在整个队列中,V-CBA组调整后的24个月随访累积平均住院费用(99087美元)显著低于rhBMP-2组(124389美元;P<0.0001),并且在单节段队列中这种模式依然存在(V-CBA组为104906美元,rhBMP-2组为125311美元;P = 0.0006)。在两个队列中,调整后的累积平均住院时间在组间均无差异。随访再入院率的差异与最初报告的初次手术的基线合并症一致。在整个队列中,V-CBA患者随后的腰椎融合率显著较低(10.12%对12.00%;P = 0.0002),而在单节段队列中两组相似,尽管V-CBA患者的基线合并症发生率显著较高,这可能对包括骨融合在内的临床结果产生负面影响。
本研究结果表明,在美国进行的腰椎融合手术中,使用V-CBA与rhBMP-2相比,24个月随访住院费用显著更低,两者随后的腰椎融合手术率和潜在相关再入院率相似。