Chemical and Biomolecular Engineering, Institute for NanoBioTechnology, Johns Hopkins University, Baltimore, Maryland.
Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University, Baltimore, Maryland.
J Nucl Med. 2022 Aug;63(8):1223-1230. doi: 10.2967/jnumed.121.262992. Epub 2021 Nov 18.
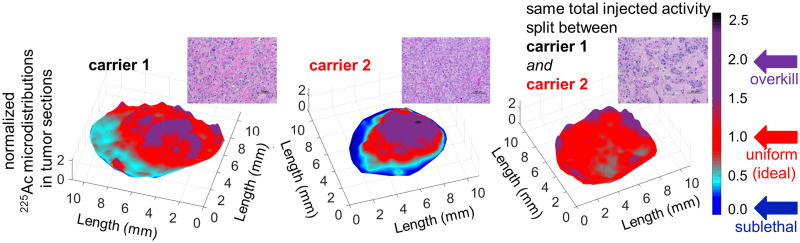
α-particle radiotherapy has already been shown to be impervious to most resistance mechanisms. However, in established (i.e., large, vascularized) soft-tissue lesions, the diffusion-limited penetration depths of radiolabeled antibodies or nanocarriers (≤50-80 μm) combined with the short range of α-particles (4-5 cell diameters) may result in only partial tumor irradiation, potentially limiting treatment efficacy. To address this challenge, we combined carriers with complementary intratumoral microdistributions of the delivered α-particles. We used the α-particle generator Ac, and we combined a tumor-responsive liposome (which, on tumor uptake, releases into the interstitium a highly diffusing form of its radioactive payload [Ac-DOTA], potentially penetrating the deeper parts of tumors where antibodies do not reach) with a separately administered, less-penetrating radiolabeled antibody (irradiating the tumor perivascular regions where liposome contents clear too quickly). In a murine model with orthotopic human epidermal growth factor receptor 2-positive BT474 breast cancer xenografts, the biodistributions of each carrier were evaluated, and the control of tumor growth was monitored after administration of the same total radioactivity of Ac delivered by the Ac-DOTA-encapsulating liposomes, by the Ac-DOTA-SCN--labeled trastuzumab, and by both carriers at equally split radioactivities. Tumor growth was significantly more inhibited when the same total injected radioactivity was divided between the 2 separate carriers than when delivered by either of the carriers alone. The combined carriers enabled more uniform intratumoral microdistributions of α-particles, at a tumor dose that was lower than the dose delivered by the antibody alone. This strategy demonstrates that more uniform microdistributions of the delivered α-particles within established solid tumors improve efficacy even at lower tumor doses. Augmentation of antibody-targeted α-particle therapies with tumor-responsive liposomes may address partial tumor irradiation, improving therapeutic effects.
α-粒子放疗已被证明不受大多数耐药机制的影响。然而,在已建立的(即大的、血管化的)软组织病变中,放射性标记的抗体或纳米载体的扩散受限穿透深度(≤50-80μm)与α-粒子的短射程(4-5 个细胞直径)相结合,可能导致肿瘤仅部分照射,从而限制了治疗效果。为了解决这一挑战,我们将载体与所递送的α-粒子的互补肿瘤内微分布相结合。我们使用α-粒子发生器 Ac,我们将一种肿瘤反应性脂质体(在肿瘤摄取后,将其放射性有效载荷的高度扩散形式[Ac-DOTA]释放到间质中,可能穿透抗体无法到达的肿瘤深部)与单独给予的、穿透性较低的放射性标记抗体(照射脂质体内容物清除过快的肿瘤血管周围区域)相结合。在具有同源人表皮生长因子受体 2 阳性 BT474 乳腺癌异种移植的小鼠模型中,评估了每种载体的生物分布,并在通过包裹 Ac-DOTA 的脂质体、Ac-DOTA-SCN--标记的曲妥珠单抗和等量放射性活性的两种载体递送相同的总放射性活性 Ac 后监测肿瘤生长的控制情况。当相同的总注入放射性活性在两种载体之间分配时,肿瘤生长的抑制明显更为显著,而不是单独使用任何一种载体时。与单独使用任何一种载体相比,联合载体使α-粒子在肿瘤内的微分布更加均匀,肿瘤剂量低于单独使用抗体时的剂量。该策略表明,即使在较低的肿瘤剂量下,在已建立的实体瘤中更均匀地分布所递送的α-粒子也可以提高疗效。用肿瘤反应性脂质体增强抗体靶向的α-粒子疗法可能会解决部分肿瘤照射问题,从而改善治疗效果。