Urology, Andrology, Renal Transplant Unit, Hôpital Pasteur 2, CHU de Nice, Nice, France.
Department of Urology and Organ Transplantation, University of Foggia, Foggia, Italy.
Immun Inflamm Dis. 2022 Feb;10(2):225-234. doi: 10.1002/iid3.566. Epub 2021 Nov 18.
Various surgical centers tend to postpone a kidney transplantation (KT) to the following morning than to operate at night-time. The objective of our study was to assess whether there was any difference between daytime and night-time renal transplantation in our institution.
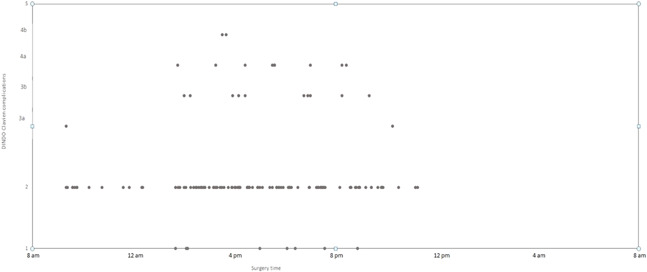
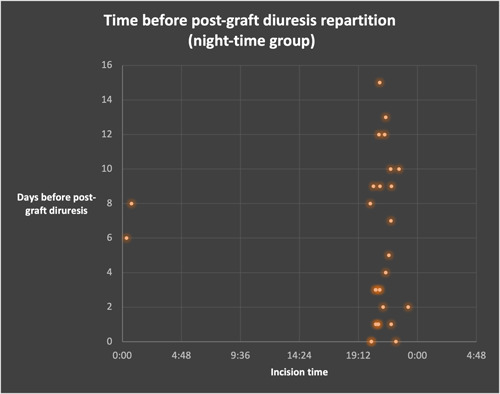
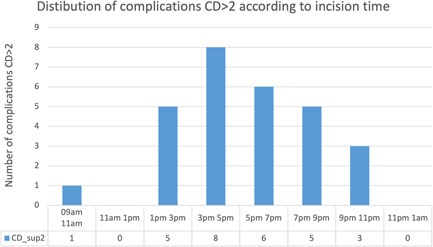
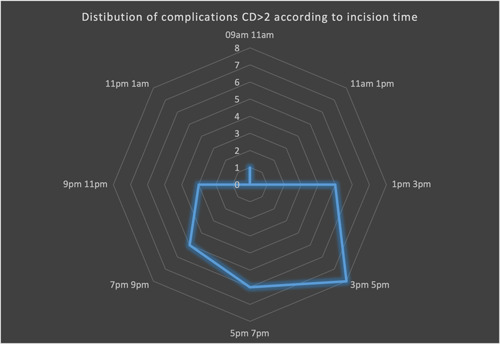
This study is a retrospective monocentric study including all the KTs that were performed between 2012 and 2013 by transplant expert surgeons in our institution. Clavien-Dindo (CD) complications were classified according to 7 variables going from 1 to 5. Time before postgraft diuresis and delayed graft function (DGF) were also analyzed. Two groups of patients were formed according to threshold value of incision time (6.30 p.m.). Data comparison were performed using the Kruskal-Wallis nonparametric test.
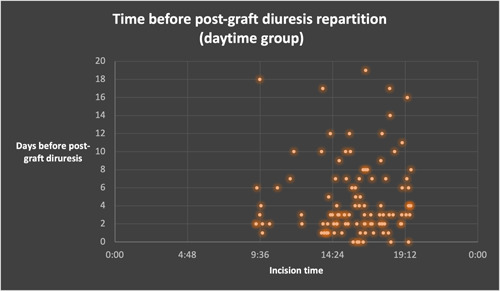
A total of 179 patients were included. Median follow-up was 24 months. Cold ischemia time was longer in the night-time transplantation (1082 vs. 807 min, p < .001), but rewarming time was shorter (47.24 vs. 52.15 min, p = .628). No statistically significant differences were observed between the two groups using the Kruskal-Wallis method for CD complications (Qobs: 0.076; p = .735). CD complications proportion was similar, with a majority of grade II complications (72.7% daytime group vs. 75.4% night-time group (p = .735). DGF (19 patients for daytime group vs. 13 patients for night-time group, p = .359) and time before postgraft diuresis (4.65 days daytime group vs. 5.27 days night-time group, p = .422) were similar between both groups. Multivariate analysis did not show significant predictors of CD complications Grade 3 and more.
Night-time renal transplantation did not induce more postoperative CD complications than diurnal procedures in our cohort, challenging the false preconceptions that allow surgical teams to delay this surgery.
许多外科中心倾向于将肾脏移植(KT)推迟到第二天早上进行,而不是在夜间进行。我们的研究目的是评估我们机构在日间和夜间进行肾脏移植是否存在差异。
这是一项回顾性单中心研究,纳入了 2012 年至 2013 年间由我们机构的移植专家外科医生进行的所有 KT。Clavien-Dindo(CD)并发症根据 7 个变量从 1 级到 5 级进行分类。还分析了移植后利尿开始前的时间和延迟移植物功能(DGF)。根据切口时间的阈值(下午 6.30)将两组患者进行分组。使用 Kruskal-Wallis 非参数检验进行数据比较。
共纳入 179 例患者。中位随访时间为 24 个月。夜间移植的冷缺血时间较长(1082 分钟 vs. 807 分钟,p < 0.001),但复温时间较短(47.24 分钟 vs. 52.15 分钟,p = 0.628)。使用 Kruskal-Wallis 方法,两组间 CD 并发症无统计学差异(Qobs:0.076;p = 0.735)。CD 并发症的比例相似,大多数为 II 级并发症(日间组 72.7% vs. 夜间组 75.4%(p = 0.735)。DGF(日间组 19 例 vs. 夜间组 13 例,p = 0.359)和移植后利尿开始前的时间(日间组 4.65 天 vs. 夜间组 5.27 天,p = 0.422)在两组间相似。多变量分析未显示 CD 并发症 3 级及以上的显著预测因子。
在我们的队列中,夜间肾脏移植并未导致术后 CD 并发症多于日间手术,这挑战了允许外科团队推迟这种手术的错误先入之见。