Department of Obstetrics and Gynecology, Stanford University, Stanford, CA; California Maternal Quality Care Collaborative, Stanford University, Stanford, CA.
Department of Obstetrics and Gynecology, Stanford University, Stanford, CA; California Maternal Quality Care Collaborative, Stanford University, Stanford, CA.
Am J Obstet Gynecol MFM. 2022 Mar;4(2):100530. doi: 10.1016/j.ajogmf.2021.100530. Epub 2021 Nov 16.
A recently developed obstetrical comorbidity scoring system enables the comparison of severe maternal morbidity rates independent of health status at the time of birth hospitalization. However, the scoring system has not been evaluated in racial-ethnic and socioeconomic groups or used to assess disparities in severe maternal morbidity.
This study aimed to evaluate the performance of an obstetrical comorbidity scoring system when applied across racial-ethnic and socioeconomic groups and to determine the effect of comorbidity score risk adjustment on disparities in severe maternal morbidity.
We analyzed a population-based cohort of live births that occurred in California during 2011 through 2017 with linked birth certificates and birth hospitalization discharge data (n=3,308,554). We updated a previously developed comorbidity scoring system to include the International Classification of Diseases, Ninth and Tenth Revisions, Clinical Modifications diagnosis codes and applied the scoring system to subpopulations (groups) defined by race-ethnicity, nativity, payment method, and educational attainment. We then calculated the risk-adjusted rates of severe maternal morbidity (including and excluding blood transfusion-only cases) for each group and estimated the disparities for these outcomes before and after adjustment for the comorbidity score using logistic regression.
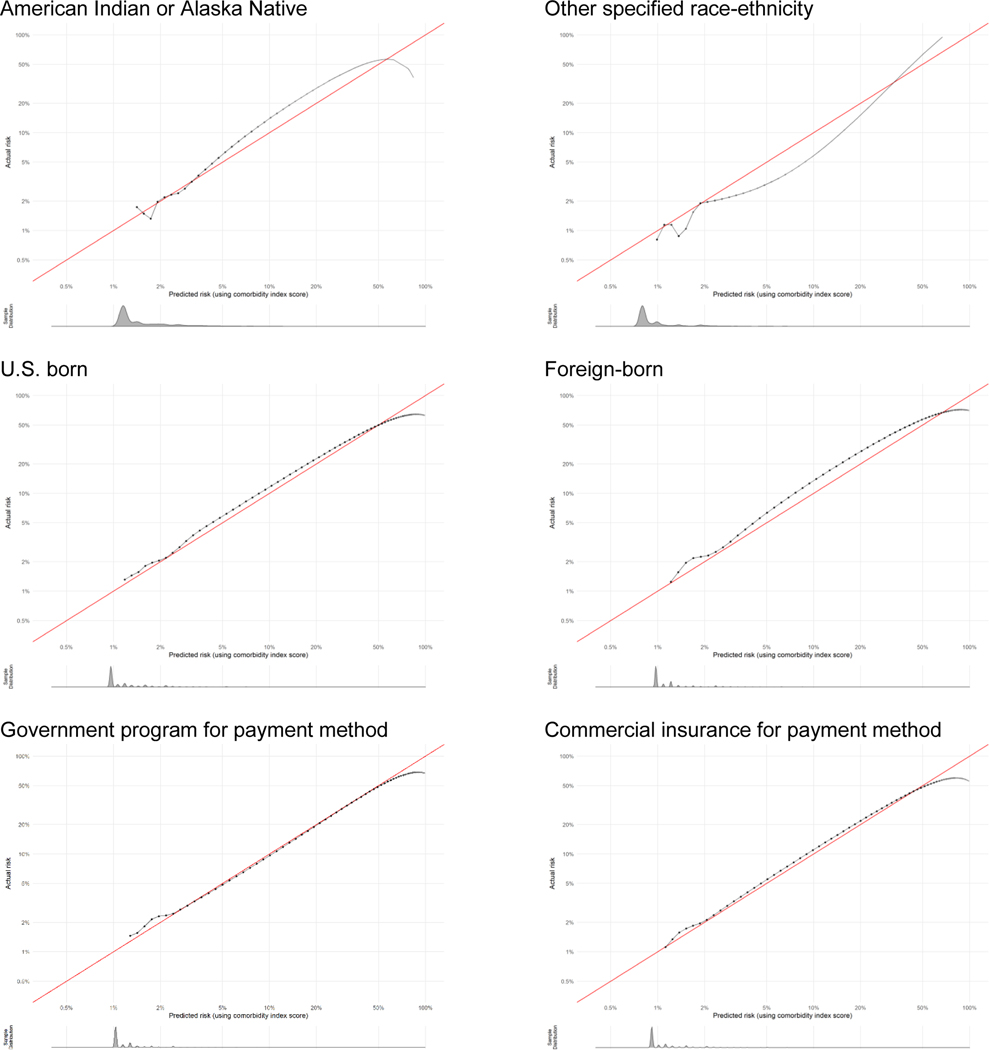
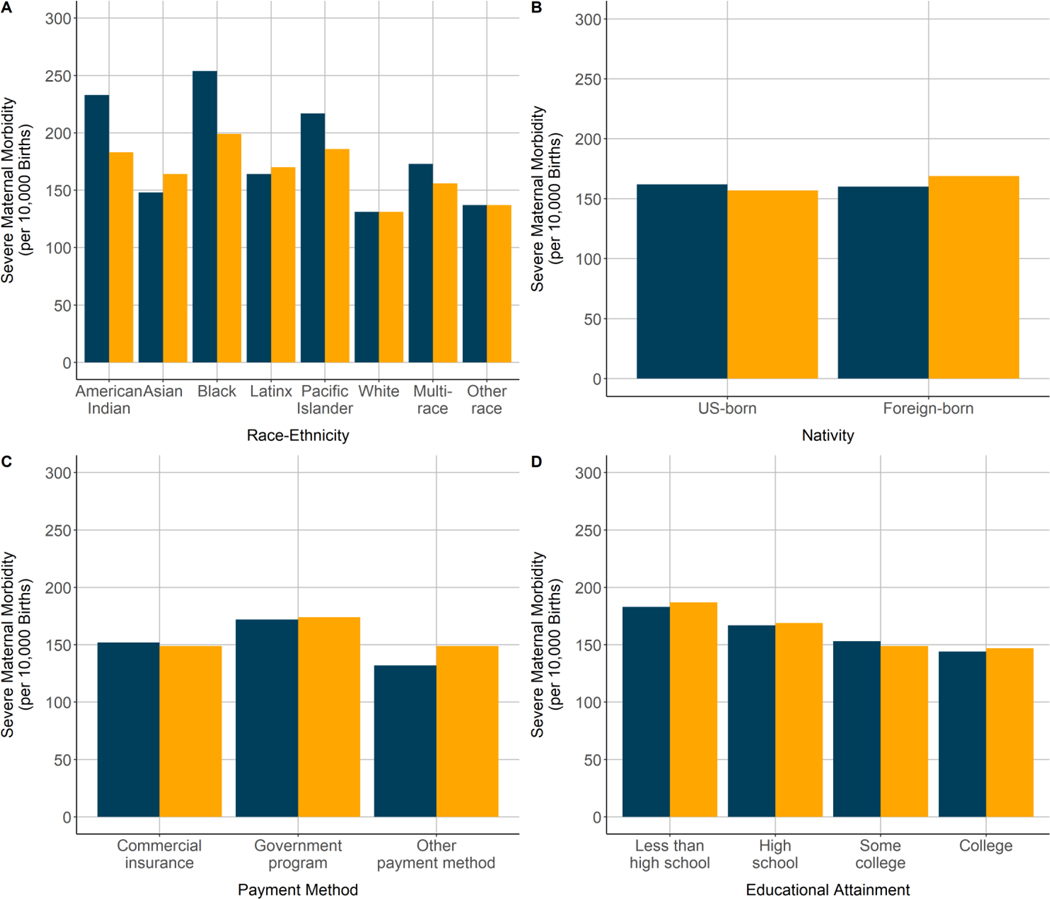
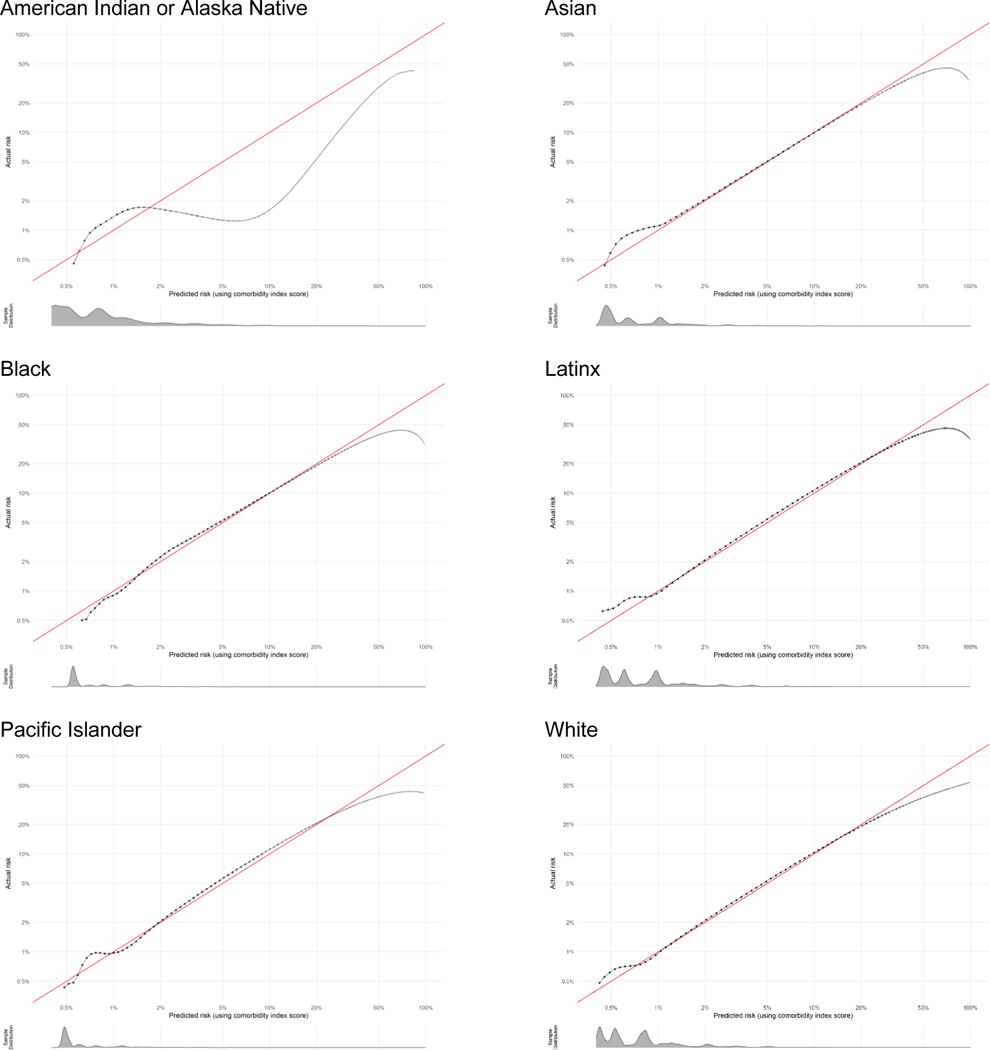
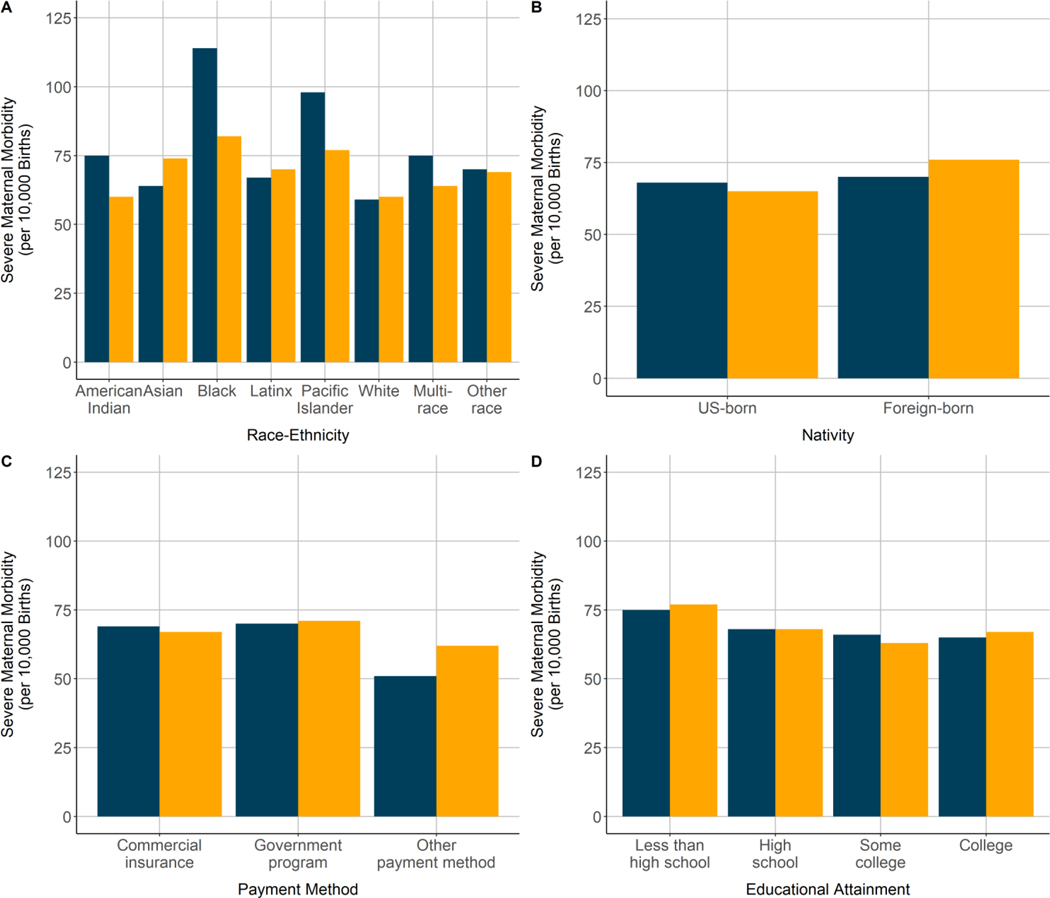
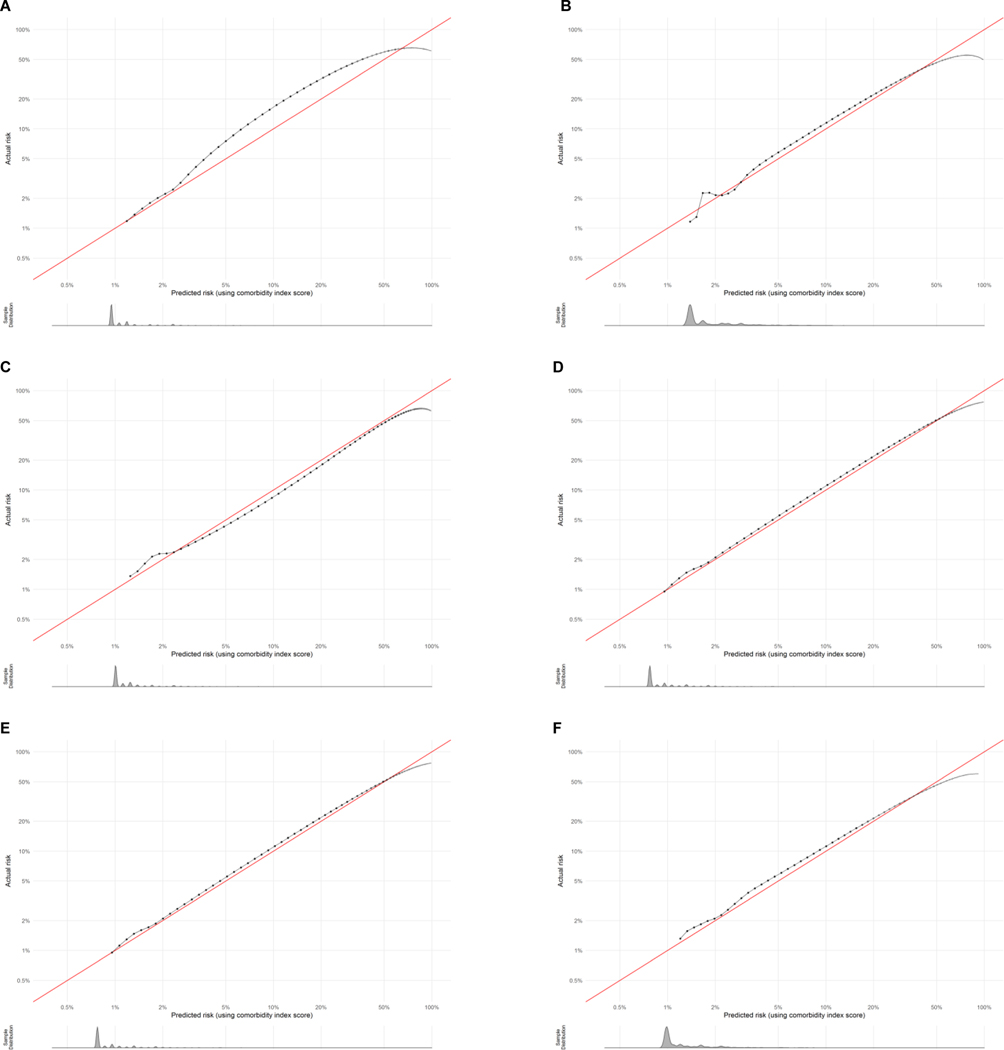
The obstetric comorbidity scores performed consistently across groups (C-statistics ranged from 0.68 to 0.76; calibration curves demonstrated overall excellent prediction of absolute risk). All non-White groups had significantly elevated rates of severe maternal morbidity before and after risk adjustment for comorbidities when compared with the White group (1.3% before, 1.3% after) (American Indian-Alaska Native: 2.1% before, 1.8% after; Asian: 1.5% before, 1.7% after; Black: 2.5% before, 2.0% after; Latinx: 1.6% before, 1.7% after; Pacific Islander: 2.2% before, 1.9% after; and multi-race groups: 1.7% before, 1.6% after). Risk adjustment also modestly increased disparities for the foreign-born group and government insurance groups. Higher educational attainment was associated with decreased severe maternal morbidity rates, which was largely unaffected by comorbidity risk adjustment. The pattern of results was the same whether or not transfusion-only cases were included as severe maternal morbidity.
These results support the use of an updated comorbidity scoring system to assess disparities in severe maternal morbidity. Disparities in severe maternal morbidity decreased in magnitude for some racial-ethnic and socioeconomic groups and increased in magnitude for other groups after adjustment for the comorbidity score.
最近开发的产科合并症评分系统可在不考虑分娩住院时健康状况的情况下比较严重产妇发病率。然而,该评分系统尚未在种族和民族以及社会经济群体中进行评估,也未用于评估严重产妇发病率的差异。
本研究旨在评估产科合并症评分系统在种族和民族以及社会经济群体中的应用表现,并确定合并症评分风险调整对严重产妇发病率差异的影响。
我们分析了加利福尼亚州 2011 年至 2017 年期间的基于人群的活产队列,这些活产与链接的出生证明和分娩住院出院数据相关(n=3,308,554)。我们更新了一个先前开发的合并症评分系统,以包含国际疾病分类,第九和第十修订版,临床修正诊断代码,并将该评分系统应用于按种族、民族、出生地、支付方式和受教育程度定义的亚人群(群体)。然后,我们计算了每个群体的严重产妇发病率(包括和不包括仅输血病例)的风险调整率,并使用逻辑回归在调整合并症评分后估计这些结局的差异。
产科合并症评分在各群体中表现一致(C 统计量范围为 0.68 至 0.76;校准曲线总体上显示了对绝对风险的出色预测)。与白人组相比,所有非白人组在调整合并症风险后,严重产妇发病率均显著升高(调整前为 1.3%,调整后为 1.3%)(美洲印第安人-阿拉斯加原住民:调整前为 2.1%,调整后为 1.8%;亚洲人:调整前为 1.5%,调整后为 1.7%;黑人:调整前为 2.5%,调整后为 2.0%;拉丁裔:调整前为 1.6%,调整后为 1.7%;太平洋岛民:调整前为 2.2%,调整后为 1.9%;多族裔群体:调整前为 1.7%,调整后为 1.6%)。风险调整也略微增加了外国出生群体和政府保险群体的差异。较高的受教育程度与严重产妇发病率降低相关,而这在很大程度上不受合并症风险调整的影响。是否包括仅输血病例作为严重产妇发病率,结果模式相同。
这些结果支持使用更新的合并症评分系统来评估严重产妇发病率的差异。在调整合并症评分后,一些种族和民族以及社会经济群体的严重产妇发病率差异有所缩小,而其他群体的差异有所扩大。