Zeng Caiwu, Li Xiaomi, Dai Yan, Zhou Ye, Li Chenglong, Liu Nan, Wang Jiangang
Center for Cardiac Intensive Care, Beijing Anzhen Hospital, Capital Medical University, No.2 Anzhen Road, Chaoyang District, Beijing, 100029, People's Republic of China.
Department of Cardiac Surgery, Beijing Anzhen Hospital, Capital Medical University, No.2 Anzhen Road, Chaoyang District, Beijing, 100029, Republic of China.
J Cardiothorac Surg. 2021 Nov 21;16(1):334. doi: 10.1186/s13019-021-01716-3.
This retrospective study sought to evaluate the efficacy of transit time flow measurement (TTFM) as a means of predicting bypass graft patency as assessed by coronary artery angiography upon 5-year follow-up.
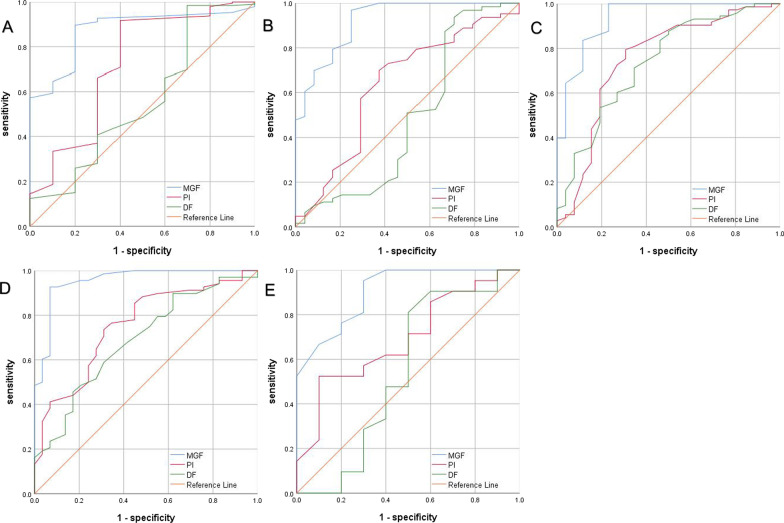
Of 311 patients undergone isolated off-pump coronary artery bypass graft surgery from January 2014 through December 2014, 202 (65%) underwent both intraoperative TTFM and angiography at follow-up. 610 grafts, 202 left internal mammary artery grafts and 408 saphenous vein grafts were checked. Any grafts that exhibited Fitzgibbon type B or O lesions upon angiographic evaluation were considered to be failing. Receiver operating characteristic curves were used to identify the optimal TTFM values for predicting graft patency.
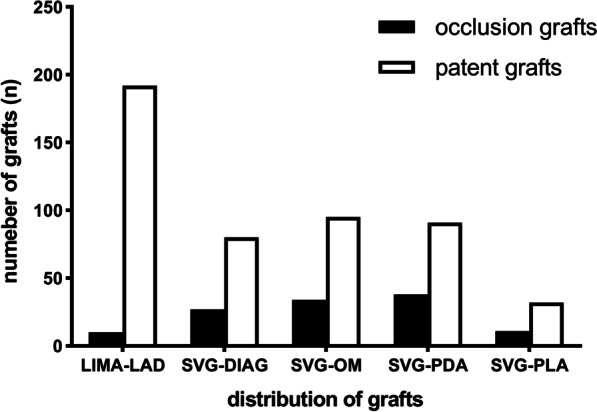
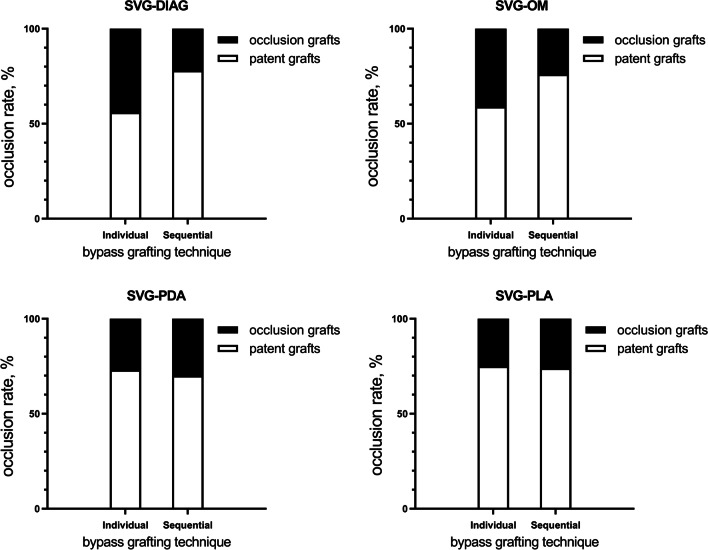
A total of 610 grafts were included in this analysis, including 202 LIMA grafts and 408 SV grafts, of which 107, 129, 129, and 43 anastomosed to DIAG, OM, PDA, and PLA, respectively. LIMA, DIAG, OM, PDA, and PLA bypass grafts had overall patency rates of 95.0%, 74.8%, 73.6%, 71.5%, and 74.4%, respectively, upon 5-year follow up. No significant differences in TTFM values (MGF, PI, and DF) were observed when comparing outcomes associated with individual or sequential SV grafting. MGF was found to be predictive of graft failure regardless of the target vessel (P < 0.05). While PI was found to predict LIMA, OM, and PDA graft failure (P < 0.05), it was not associated with the failure of grafts associated with DIAG and PLA vessels. Similarly, DF was found to predict OM and PDA graft failure (P < 0.05), but was not significantly associated with the failure of grafts associated with LIMA, DIAG, or PLA vessels.
LIMA bypass grafts were associated with better 5-year graft patency relative to SV bypass grafts. Similar graft patency rates were observed for both individual and sequential bypass grafts. MGF was able to predict bypass graft failure in patients that underwent off-pump CABG surgery.
本回顾性研究旨在评估通过冠状动脉造影术在5年随访时评估的通过时间流量测量(TTFM)作为预测旁路移植血管通畅性方法的有效性。
在2014年1月至2014年12月接受非体外循环冠状动脉旁路移植手术的311例患者中,202例(65%)在随访时接受了术中TTFM和血管造影检查。检查了610条移植血管,其中202条左乳内动脉移植血管和408条大隐静脉移植血管。血管造影评估显示为菲茨吉本B型或O型病变的任何移植血管被视为失败。采用受试者工作特征曲线确定预测移植血管通畅性的最佳TTFM值。
本分析共纳入610条移植血管,包括202条左乳内动脉移植血管和408条大隐静脉移植血管,其中分别有107条、129条、129条和43条吻合至对角支(DIAG)、钝缘支(OM)、后降支(PDA)和左室后支(PLA)。在5年随访时,左乳内动脉、对角支、钝缘支、后降支和左室后支旁路移植血管的总体通畅率分别为95.0%、74.8%、73.6%、71.5%和74.4%。比较单个或序贯大隐静脉移植血管的相关结果时,未观察到TTFM值(平均血流速度[MGF]、搏动指数[PI]和阻力指数[DF])有显著差异。发现MGF可预测移植血管失败,无论靶血管如何(P<0.05)。虽然发现PI可预测左乳内动脉、钝缘支和后降支移植血管失败(P<0.05),但它与对角支和左室后支血管相关移植血管的失败无关。同样,发现DF可预测钝缘支和后降支移植血管失败(P<0.05),但与左乳内动脉、对角支或左室后支血管相关移植血管的失败无显著关联。
与大隐静脉旁路移植血管相比,左乳内动脉旁路移植血管在5年时具有更好的移植血管通畅性。单个和序贯旁路移植血管的移植血管通畅率相似。MGF能够预测接受非体外循环冠状动脉旁路移植手术患者的旁路移植血管失败。