Chang Wai Hoong, Mueller Stefanie H, Tan Yen Yi, Lai Alvina G
Institute of Health Informatics, University College London, London, UK.
Lancet Reg Health Eur. 2021 Sep 8;10:100222. doi: 10.1016/j.lanepe.2021.100222. eCollection 2021 Nov.
Patients with liver disease have complex haemostasis and due to such contraindications, landmark randomised controlled trials investigating antithrombotic medicines have often excluded these patients. As a result, there has been limited consensus on the safety, efficacy and monitoring practices of anticoagulant and antiplatelet therapy in patients with liver disease. This study aims to investigate prescribing prevalence, adherence, persistence and impact of adherence on bleeding and stroke risk in people with and without liver disease taking anticoagulants and antiplatelets.
We employed a population-based cohort consisting of person-level linked records from primary care, secondary care and the death registry. The cohort consisted of 3,929,596 adults aged ≥ 30 years during the study period of 1998 to 2020 and registered with an NHS general practitioner in England. The primary outcome was prescribing prevalence, adherence to and persistence with anticoagulant and antiplatelet therapy comparing patients with and without liver disease. Risk factors for non-adherence and non-persistence were analysed using multivariable logistic regression and Cox regression. Impact of adherence on bleeding and ischaemic stroke was assessed.
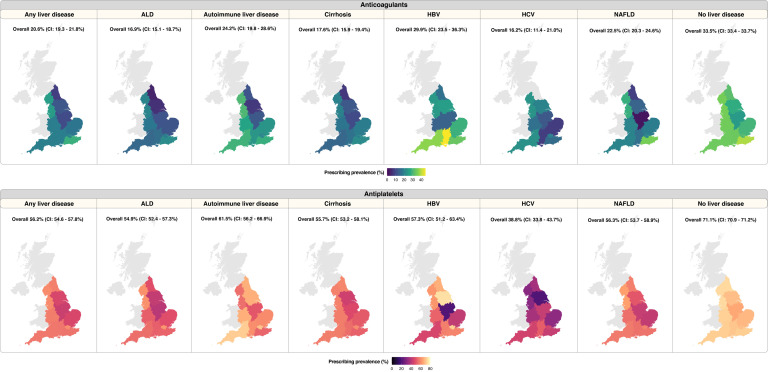
Among patients with any of the six liver diseases (ALD, autoimmune liver disease, cirrhosis, HBV, HCV and NAFLD), we identified 4,237 individuals with incident atrial fibrillation (indication for anticoagulants) and 4,929 individuals with incident myocardial infarction, transient ischaemic attack, unstable angina or peripheral arterial disease (indication for antiplatelets). Among patients without liver disease, 321,510 and 386,643 individuals were identified as having indications for anticoagulant and antiplatelet therapy, respectively. Among drug-naïve individuals, prescribing prevalence was lower in patients with liver disease compared with individuals without liver disease: anticoagulants (20.6% [806/3,921] vs. 33.5% [103,222/307,877]) and antiplatelets (56.2% [2,207/3,927] vs. 71.1% [249,258/350,803]). Primary non-adherence rates (stopping after one prescription) were higher in patients with liver disease, compared with those without liver disease: anticoagulants (7.9% [64/806] vs. 4.7% [4,841/103,222]) and antiplatelets (6.2% [137/2,207] vs. 4.4% [10,993/249,258]). Among individuals who were not primary non-adherent and had at least 12 months of follow-up, patients with liver disease however had a higher one-year adherence rate: anticoagulants (33.1% [208/628] vs. 29.4% [26,615/90,569]) and antiplatelets (40.9% [743/1,818] vs. 34.4% [76,834/223,154]). Likelihood of non-adherence was lower in apixaban and rivaroxaban (relative to warfarin) and lower in clopidogrel (relative to aspirin). Increased comorbidity burden (by CHADSVASc score) was associated with decreased risk of non-adherence and non-persistence with anticoagulants. Overall rates of 'non-adherent, non-persistent' were highest in warfarin (compared with apixaban and rivaroxaban) and aspirin (compared with clopidogrel or dipyridamole) in patients with and without liver disease. Among patients without liver disease, not taking antithrombotic medications for >3 months was associated with a higher risk of stroke, however, adherence to these medications was also associated with a small increase in risk of bleeding. Patients with liver disease (when compared with those without liver disease) had higher risks of stroke, especially when they stopped taking antiplatelets for >3 months. Patients with liver disease who were adherent to antiplatelets, however, had a higher risk of bleeding compared with patients without liver disease.
Use of antithrombotic medicines in patients with and without liver disease is suboptimal with heterogeneity across medicines. As patients with liver disease are excluded from major randomised trials for these drugs, our results provide real-world evidence that may inform medicine optimisation strategies. We outline challenges and opportunities for tackling non-adherence, which begins with understanding patients' views of medicines to help them make informed decisions about appropriate use.
AGL is supported by funding from the Wellcome Trust (204841/Z/16/Z), National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre (BRC714/HI/RW/101440), NIHR Great Ormond Street Hospital Biomedical Research Centre (19RX02), the Health Data Research UK Better Care Catalyst Award (CFC0125) and the Academy of Medical Sciences (SBF006\1084). The funders have no role in the writing of the manuscript or the decision to submit it for publication.
肝病患者的止血功能复杂,由于存在此类禁忌证,一些研究抗血栓药物的标志性随机对照试验常常将这些患者排除在外。因此,对于肝病患者抗凝和抗血小板治疗的安全性、有效性及监测方法,目前尚未达成广泛共识。本研究旨在调查服用抗凝药和抗血小板药物的肝病患者与非肝病患者的处方开具率、依从性、持续性以及依从性对出血和中风风险的影响。
我们采用了一个基于人群的队列,该队列由来自初级保健、二级保健和死亡登记处的个人层面关联记录组成。该队列包括在1998年至2020年研究期间年龄≥30岁且在英格兰国民保健服务(NHS)全科医生处注册的3,929,596名成年人。主要结局是比较肝病患者与非肝病患者抗凝和抗血小板治疗的处方开具率、依从性和持续性。使用多变量逻辑回归和Cox回归分析不依从和不持续的危险因素。评估依从性对出血和缺血性中风的影响。
在患有六种肝病(酒精性肝病、自身免疫性肝病、肝硬化、乙肝、丙肝和非酒精性脂肪性肝病)中的任何一种的患者中,我们确定了4237例新发房颤患者(抗凝治疗指征)和4929例新发心肌梗死、短暂性脑缺血发作、不稳定型心绞痛或外周动脉疾病患者(抗血小板治疗指征)。在无肝病患者中,分别有321,510例和386,643例被确定有抗凝和抗血小板治疗指征。在未用过药的个体中,肝病患者的处方开具率低于非肝病患者:抗凝药(20.6%[806/3921]对33.5%[103,222/307,877])和抗血小板药(56.2%[2207/3927]对71.1%[249,258/350,803])。与非肝病患者相比,肝病患者的初次不依从率(一剂处方后停药)更高:抗凝药(7.9%[64/806]对4.7%[4841/103,222])和抗血小板药(6.2%[137/2207]对4.4%[10,993/249,258])。然而,在非初次不依从且至少随访12个月的个体中,肝病患者的一年依从率更高:抗凝药(33.1%[208/628]对29.4%[26,615/90,569])和抗血小板药(40.9%[743/1818]对34.4%[76,834/223,154])。阿哌沙班和利伐沙班(相对于华法林)的不依从可能性较低,氯吡格雷(相对于阿司匹林)的不依从可能性较低。合并症负担增加(通过CHADSVASc评分)与抗凝药不依从和不持续风险降低相关。在有肝病和无肝病的患者中,“不依从、不持续”的总体发生率在华法林(与阿哌沙班和利伐沙班相比)和阿司匹林(与氯吡格雷或双嘧达莫相比)中最高。在无肝病患者中,未服用抗血栓药物超过3个月与中风风险较高相关,然而,坚持服用这些药物也与出血风险略有增加相关。肝病患者(与无肝病患者相比)中风风险更高,尤其是当他们停止服用抗血小板药物超过3个月时。然而,坚持服用抗血小板药物的肝病患者与无肝病患者相比出血风险更高。
无论有无肝病,抗血栓药物的使用都不理想,不同药物之间存在异质性。由于肝病患者被排除在这些药物的主要随机试验之外,我们的结果提供了真实世界的证据,可为药物优化策略提供参考。我们概述了解决不依从问题的挑战和机遇,这首先要了解患者对药物的看法,以帮助他们就合理用药做出明智的决定。
AGL得到了惠康信托基金(204841/Z/16/Z)、国家卫生研究院(NIHR)伦敦大学学院医院生物医学研究中心(BRC714/HI/RW/101440)、NIHR大奥蒙德街医院生物医学研究中心(19RX02)、英国健康数据研究更好护理催化剂奖(CFC0125)和医学科学院(SBF006\1084)的资助。资助者在撰写本文或决定提交发表方面没有任何作用。

