French National Health Insurance (Caisse Nationale de L'Assurance Maladie, Cnam), 50 Avenue du Pr. André Lemierre, 75 986, Paris Cedex 20, France.
Clinical Investigation Center, Clinical Epidemiology/Clinical Trials Unit, Dijon-Bourgogne University Hospital, 21 000, Dijon, France.
Sci Rep. 2020 Jul 15;10(1):11624. doi: 10.1038/s41598-020-68304-8.
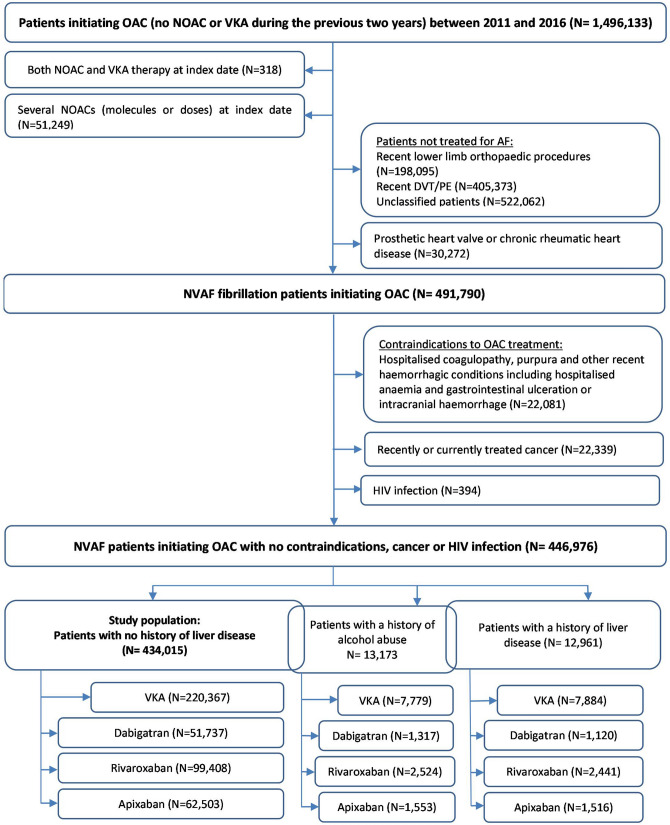
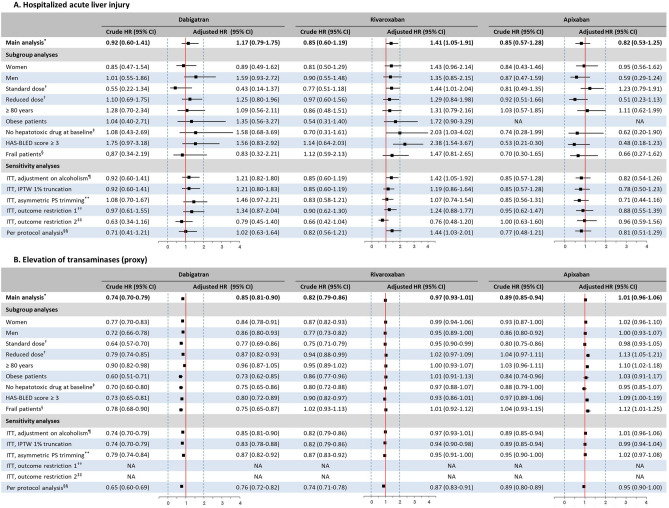
Insufficient real-world data on acute liver injury (ALI) risk associated with oral anticoagulants (OACs) exist in patients with nonvalvular atrial fibrillation (NVAF). Using the French national healthcare databases, a propensity-weighted nationwide cohort study was performed in NVAF patients initiating OACs from 2011 to 2016, considering separately those (1) with no prior liver disease (PLD) as main population, (2) with PLD, (3) with a history of chronic alcoholism. A Cox proportional hazards model was used to estimate the hazard ratio with 95% confidence interval (HR [95% CI]) of serious ALI (hospitalised ALI or liver transplantation) during the first year of treatment, for each non-vitamin K antagonist (VKA) oral anticoagulant (NOAC: dabigatran, rivaroxaban, apixaban) versus VKA. In patients with no PLD (N = 434,015), only rivaroxaban new users were at increased risk of serious ALI compared to VKA initiation (adjusted HR: 1.41 [1.05-1.91]). In patients with chronic alcoholism history (N = 13,173), only those initiating dabigatran were at increased risk of serious ALI compared to VKA (2.88 [1.74-4.76]) but an ancillary outcome suggested that differential clinical follow-up between groups might partly explain this association. In conclusion, this study does not suggest an increase of the 1-year risk of ALI in NOAC versus VKA patients with AF.
在非瓣膜性心房颤动(NVAF)患者中,关于口服抗凝剂(OACs)相关急性肝损伤(ALI)风险的真实世界数据不足。本研究使用法国国家医疗保健数据库,在 2011 年至 2016 年间对开始使用 OAC 的 NVAF 患者进行了一项倾向评分加权的全国性队列研究,分别考虑了(1)无既往肝脏疾病(PLD)的患者(主要人群)、(2)有 PLD 的患者和(3)有慢性酒精中毒史的患者。采用 Cox 比例风险模型,对每个非维生素 K 拮抗剂(VKA)口服抗凝剂(NOAC:达比加群、利伐沙班、阿哌沙班)与 VKA 相比,在治疗的第一年中严重 ALI(住院 ALI 或肝移植)的风险比(HR [95%CI])进行了估计。在无 PLD 的患者中(N=434,015),与 VKA 起始相比,只有利伐沙班新使用者发生严重 ALI 的风险增加(校正 HR:1.41 [1.05-1.91])。在有慢性酒精中毒史的患者中(N=13,173),与 VKA 相比,只有起始使用达比加群的患者发生严重 ALI 的风险增加(2.88 [1.74-4.76]),但辅助结果表明,两组之间的差异临床随访可能部分解释了这种关联。总之,这项研究并未表明与 AF 患者相比,NOAC 与 VKA 相比,1 年内 ALI 的风险增加。