Zhang Sirui, Li Yupei, Liu Guina, Su Baihai
West China School of Medicine, Sichuan University, 610041, Chengdu, China.
Department of Nephrology, Med+ Biomaterial Institute, West China Hospital, Sichuan University, 610041, Chengdu, China.
Thromb J. 2021 Nov 24;19(1):91. doi: 10.1186/s12959-021-00343-1.
Anticoagulation in hospitalized COVID-19 patients has been associated with survival benefit; however, the optimal anticoagulant strategy has not yet been defined. The objective of this meta-analysis was to investigate the effect of intermediate-to-therapeutic versus prophylactic anticoagulation for thromboprophylaxis on the primary outcome of in-hospital mortality and other patient-centered secondary outcomes in COVID-19 patients.
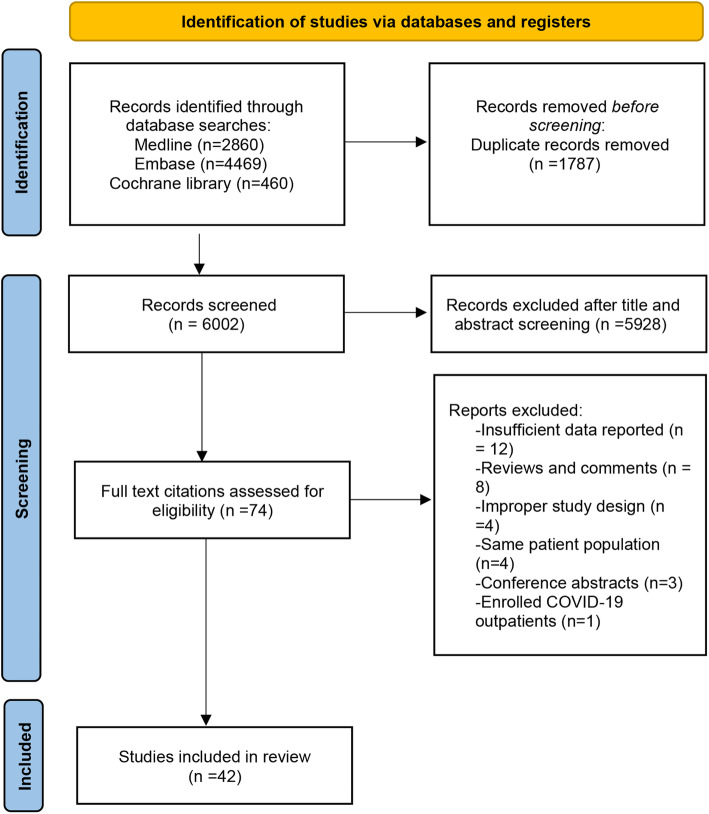
MEDLINE, EMBASE, and Cochrane databases were searched from inception to August 10th 2021. Cohort studies and randomized clinical trials that assessed the efficacy and safety of intermediate-to-therapeutic versus prophylactic anticoagulation in hospitalized COVID-19 patients were included. Baseline characteristics and relevant data of each study were extracted in a pre-designed standardized data-collection form. The primary outcome was all-cause in-hospital mortality and the secondary outcomes were incidence of thrombotic events and incidence of any bleeding and major bleeding. Pooled analysis with random effects models yielded relative risk with 95 % CIs.
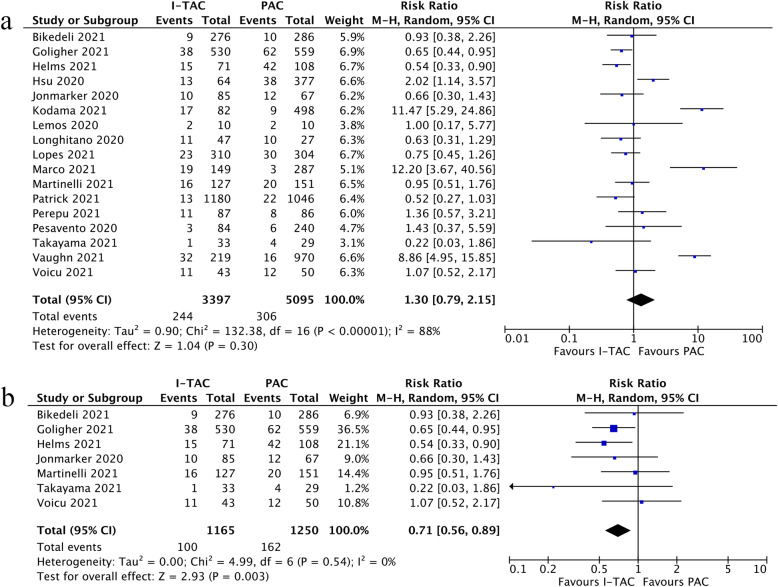
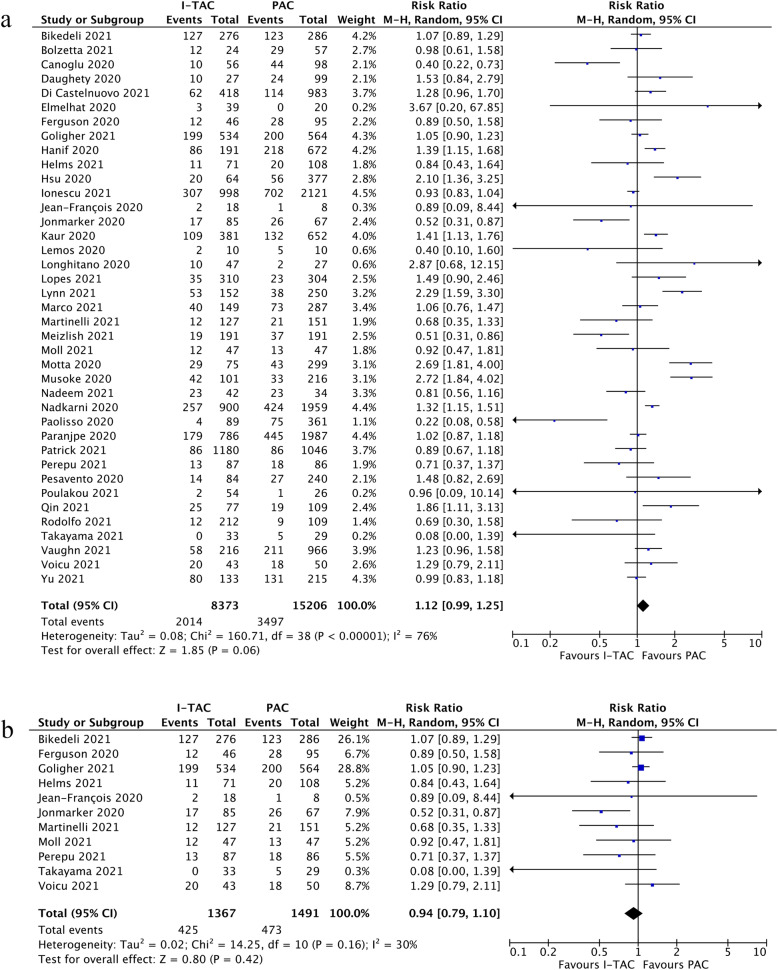
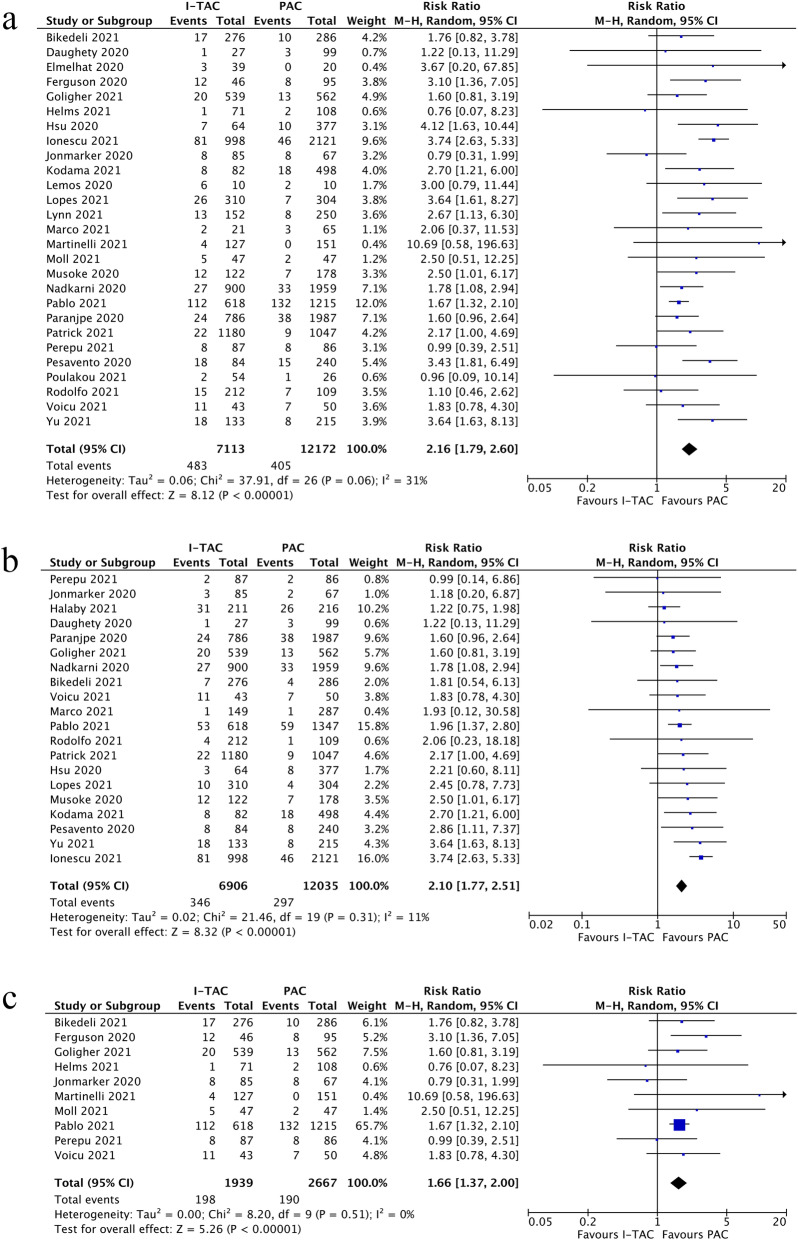
This meta-analysis included 42 studies with 28,055 in-hospital COVID-19 patients totally. Our pooled analysis demonstrated that intermediate-to-therapeutic anticoagulation was not associated with lower in-hospital mortality (RR=1.12, 95 %CI 0.99-1.25, p=0.06, I=77 %) and lower incidence of thrombotic events (RR=1.30, 95 %CI 0.79-2.15, p=0.30, I=88 %), but increased the risk of any bleeding events (RR=2.16, 95 %CI 1.79-2.60, p<0.01, I=31 %) and major bleeding events significantly (RR=2.10, 95 %CI 1.77-2.51, p<0.01, I=11 %) versus prophylactic anticoagulation. Moreover, intermediate-to-therapeutic anticoagulation decreased the incidence of thrombotic events (RR=0.71, 95 %CI 0.56-0.89, p=0.003, I=0 %) among critically ill COVID-19 patients admitted to intensive care units (ICU), with increased bleeding risk (RR=1.66, 95 %CI 1.37-2.00, p<0.01, I=0 %) and unchanged in-hospital mortality (RR=0.94, 95 %CI 0.79-1.10, p=0.42, I=30 %) in such patients. The Grading of Recommendation, Assessment, Development, and Evaluation certainty of evidence ranged from very low to moderate.
We recommend the use of prophylactic anticoagulation against intermediate-to-therapeutic anticoagulation among unselected hospitalized COVID-19 patients considering insignificant survival benefits but higher risk of bleeding in the escalated thromboprophylaxis strategy. For critically ill COVID-19 patients, the benefits of intermediate-to-therapeutic anticoagulation in reducing thrombotic events should be weighed cautiously because of its association with higher risk of bleeding.
The protocol was registered at PROSPERO on August 17th 2021 ( CRD42021273780 ).
住院的新冠病毒疾病(COVID-19)患者进行抗凝治疗与生存获益相关;然而,最佳的抗凝策略尚未明确。本荟萃分析的目的是研究中度至治疗性抗凝与预防性抗凝在预防血栓形成方面对COVID-19患者的院内死亡率这一主要结局以及其他以患者为中心的次要结局的影响。
检索MEDLINE、EMBASE和Cochrane数据库,检索时间从数据库建立至2021年8月10日。纳入评估中度至治疗性抗凝与预防性抗凝在住院COVID-19患者中的疗效和安全性的队列研究和随机临床试验。每项研究的基线特征和相关数据通过预先设计的标准化数据收集表提取。主要结局是全因院内死亡率,次要结局是血栓形成事件的发生率、任何出血和大出血的发生率。采用随机效应模型进行汇总分析,得出相对风险及95%置信区间。
本荟萃分析共纳入42项研究,总计28055例住院COVID-19患者。我们的汇总分析表明,与预防性抗凝相比,中度至治疗性抗凝与较低的院内死亡率(相对风险[RR]=1.12,95%置信区间[CI] 0.99 - 1.25,p = 0.06,I² = 77%)和较低的血栓形成事件发生率(RR = 1.30,95%CI 0.79 - 2.15,p = 0.30,I² = 88%)无关,但会显著增加任何出血事件(RR = 2.16,95%CI 1.79 - 2.60,p < 0.01,I² = 31%)和大出血事件的风险(RR = 2.10,95%CI 1.77 - 2.51,p < 0.01,I² = 11%)。此外,对于入住重症监护病房(ICU)的重症COVID-19患者,中度至治疗性抗凝可降低血栓形成事件的发生率(RR = 0.71,95%CI 0.56 - 0.89,p = 0.003,I² = 0%),但此类患者的出血风险增加(RR = 1.66,95%CI 1.37 - 2.00,p < 0.01,I² = 0%),院内死亡率无变化(RR = 0.94,95%CI 0.79 - 1.10,p = 0.42,I² = 30%)。证据的推荐分级、评估、制定和评价确定性从极低到中等不等。
考虑到在未选择的住院COVID-19患者中,升级的血栓预防策略生存获益不显著但出血风险更高,我们建议采用预防性抗凝而非中度至治疗性抗凝。对于重症COVID-19患者,由于中度至治疗性抗凝与较高的出血风险相关,在降低血栓形成事件方面的益处应谨慎权衡。
该方案于2021年8月17日在国际前瞻性系统评价注册库(PROSPERO)注册(CRD42021273780)。