Chiu Tai-Jan, Su Yung-Yeh, Yang Shih-Hung, Li Chung-Pin, Bai Li-Yuan, Chiang Nai-Jung, Chuang Shih-Chang, Shan Yan-Shen, Chan De-Chuan, Chen Li-Tzong, Yen Chia-Jui, Peng Cheng-Ming, Chen Yen-Yang, Chen Jen-Shi, Chou Wen-Chi
Division of Hematology-Oncology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University, Kaohsiung.
National Institute of Cancer Research, National Health Research Institutes, Tainan.
Ther Adv Med Oncol. 2021 Nov 20;13:17588359211058255. doi: 10.1177/17588359211058255. eCollection 2021.
Liposomal irinotecan (nal-IRI) plus 5-fluorouracil and leucovorin (5-FU/LV) is currently the standard second-line treatment for patients with pancreatic ductal adenocarcinoma (PDAC) after previous failed gemcitabine-based therapy. This population-based study aimed to evaluate the efficacy and safety of nal-IRI + 5-FU/LV and the association of pre-emptive nal-IRI dosing with treatment outcomes in patients with PDAC.
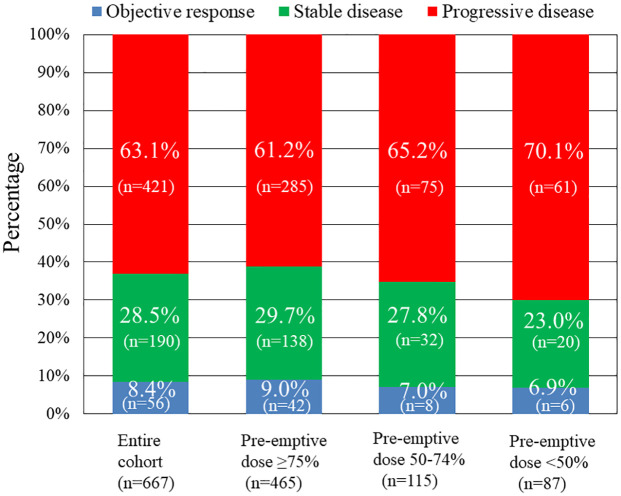
We retrospectively enrolled a total of 667 consecutive patients with PDAC who received nal-IRI plus 5-FU/LV treatment between August 2018 and November 2020 at 9 medical centers in Taiwan. Patients were allocated into groups according to pre-emptive nal-IRI dosing (⩾75%, 50-74%, <50%) for comparison of treatment efficacy and safety.
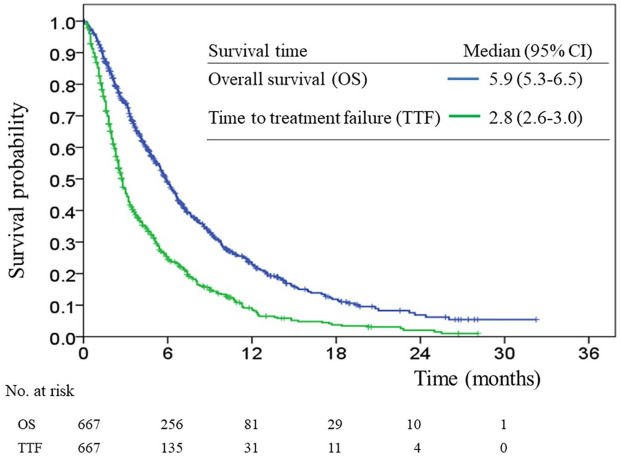
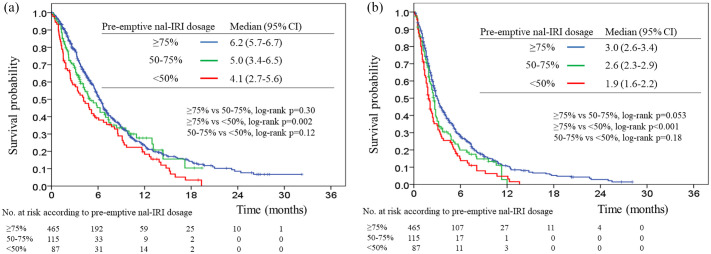
The median overall survival (OS) and time to treatment failure (TTF) were 5.9 months [95% confidence interval (CI), 5.3-6.5] and 2.8 months (95% CI, 2.6-3.0), respectively. The median OS was 6.5 months (95% CI, 5.7-6.7), 5.0 months (95% CI, 3.4-6.5), and 4.1 months (95% CI, 2.7-5.6), respectively, among the ⩾75%, 50-74%, and <50% pre-emptive nal-IRI dosing groups, whereas the median TTF of the three groups was 3.0 months (95% CI, 2.6-3.4), 2.6 months (95% CI, 2.3-2.9), and 1.9 months (95% CI, 1.6-2.2), respectively. Pre-emptive nal-IRI dosing <50% was an independent negative prognostic factor for OS and TTF in multivariate analyses. The most common severe adverse events were neutropenia (22.9%), anemia (21.1%), and hypokalemia (15.4%). Patients in the <50% pre-emptive nal-IRI dosing group had a significantly lower incidence of neutropenia and non-neutropenic infection than those in the other groups.
Our results support the use of nal-IRI + 5-FU/LV as standard clinical practice for treating patients with PDAC based on this large population-based study. Our findings encourage physicians to provide adequate doses of nal-IRI in order to achieve better outcomes without compromising safety profiles.
脂质体伊立替康(nal-IRI)联合5-氟尿嘧啶和亚叶酸钙(5-FU/LV)目前是既往基于吉西他滨的治疗失败后的胰腺导管腺癌(PDAC)患者的标准二线治疗方案。这项基于人群的研究旨在评估nal-IRI + 5-FU/LV的疗效和安全性,以及PDAC患者中预先设定的nal-IRI剂量与治疗结果之间的关联。
我们回顾性纳入了2018年8月至2020年11月期间在台湾9家医疗中心接受nal-IRI联合5-FU/LV治疗的667例连续PDAC患者。根据预先设定的nal-IRI剂量(⩾75%、50 - 74%、<50%)将患者分组,以比较治疗效果和安全性。
中位总生存期(OS)和治疗失败时间(TTF)分别为5.9个月[95%置信区间(CI),5.3 - 6.5]和2.8个月(95% CI,2.6 - 3.0)。预先设定的nal-IRI剂量⩾75%、50 - 74%和<50%的组中,中位OS分别为6.5个月(95% CI,5.7 - 6.7)、5.0个月(95% CI,3.4 - 6.5)和4.1个月(95% CI,2.7 - 5.6),而三组的中位TTF分别为3.0个月(95% CI,2.6 - 3.4)、2.6个月(95% CI,2.3 - 2.9)和1.9个月(95% CI,1.6 - 2.2)。在多因素分析中,预先设定的nal-IRI剂量<50%是OS和TTF的独立不良预后因素。最常见的严重不良事件是中性粒细胞减少(22.9%)、贫血(21.1%)和低钾血症(15.4%)。预先设定的nal-IRI剂量<50%的组中性粒细胞减少和非中性粒细胞感染的发生率明显低于其他组。
基于这项大型基于人群的研究,我们的结果支持将nal-IRI + 5-FU/LV作为治疗PDAC患者的标准临床实践。我们的发现鼓励医生提供足够剂量的nal-IRI,以便在不影响安全性的情况下取得更好的治疗效果。