Bang Kyunghye, Cheon Jaekyung, Jeong Jae Ho, Im Hyeon-Su, Kim Kyu-Pyo, Ryoo Baek-Yeol, Yoo Changhoon
Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Division of Hematology-Oncology, Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Republic of Korea.
Ther Adv Med Oncol. 2021 Mar 19;13:17588359211003053. doi: 10.1177/17588359211003053. eCollection 2021.
Liposomal irinotecan (nal-IRI) plus fluorouracil/leucovorin (5-FU/LV) has shown clinical benefit in patients with metastatic pancreatic adenocarcinoma (mPAC) who progressed on gemcitabine-based chemotherapy. However, its role in patients with mPAC previously treated with conventional irinotecan-containing chemotherapy has not been appropriately investigated.
In this retrospective analysis, patients with mPAC who received nal-IRI plus 5-FU/LV after conventional irinotecan-containing regimen between January 2017 and March 2020, were identified from two referral cancer centers in South Korea. The ratio of time to progression (TTP) with nal-IRI plus 5-FU/LV to TTP with conventional irinotecan (TTPr) was analyzed with respect to the duration and cumulative dose of conventional irinotecan treatment.
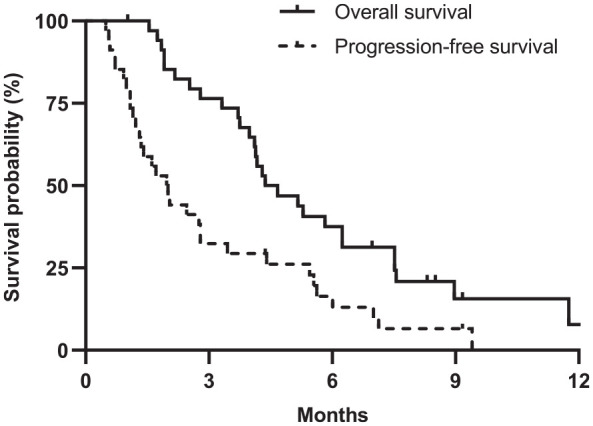
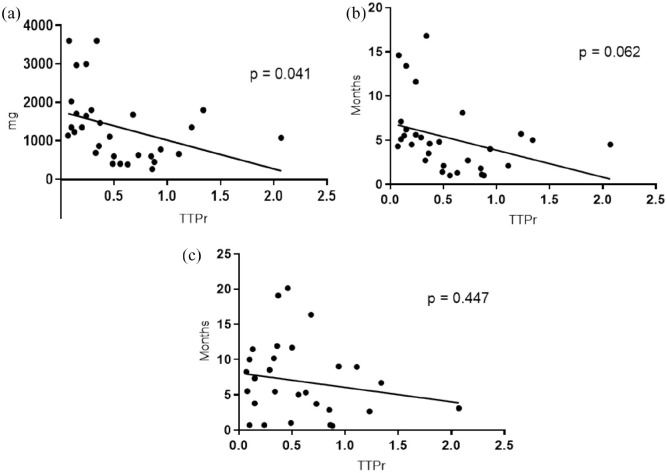
In total, 35 patients treated with nal-IRI plus 5-FU/LV after the irinotecan-containing regimen were analyzed. The median age was 58 years and 16 (46%) patients were male. The median duration of conventional irinotecan therapy was 4.6 months at a median cumulative dose of 1230 mg. The objective response rate of nal-IRI plus 5-FU/LV was 2.9%, and stable disease was achieved in 11 (31.4%) patients. During the median follow-up of 9.2 [95% confidence interval (CI): 7.8-10.5] months, the median progression-free survival (PFS) and overall survival (OS) were 2.0 (95% CI: 1.4-2.6) months and 4.4 (95% CI: 3.6-5.7) months, respectively. The 6-month PFS and OS rates were 16.3% and 37.5%, respectively. The median TTPr was 0.41 (range, 0.07-2.07), showing a negative correlation with the cumulative dose of prior irinotecan therapy (R = -0.37, = 0.041). A tentative negative correlation between TTPr and duration of prior irinotecan therapy was observed ( = -0.35, = 0.062). The most common grade 3-4 toxicities were neutropenia (20%) and fatigue (8.6%).
Nal-IRI plus 5-FU/LV showed modest effectiveness and manageable toxicities for patients with mPAC previously treated with conventional irinotecan-containing chemotherapy. The cumulative dose of prior conventional irinotecan therapy may be inversely correlated with the effectiveness of nal-IRI plus 5-FU/LV.
脂质体伊立替康(nal-IRI)联合氟尿嘧啶/亚叶酸钙(5-FU/LV)已在接受基于吉西他滨的化疗后病情进展的转移性胰腺腺癌(mPAC)患者中显示出临床获益。然而,其在先前接受过含传统伊立替康化疗的mPAC患者中的作用尚未得到充分研究。
在这项回顾性分析中,从韩国的两个转诊癌症中心确定了在2017年1月至2020年3月期间接受含传统伊立替康方案治疗后接受nal-IRI联合5-FU/LV治疗的mPAC患者。分析了nal-IRI联合5-FU/LV的疾病进展时间(TTP)与传统伊立替康的TTP之比(TTPr)与传统伊立替康治疗的持续时间和累积剂量的关系。
总共分析了35例在含伊立替康方案后接受nal-IRI联合5-FU/LV治疗的患者。中位年龄为58岁,16例(46%)患者为男性。传统伊立替康治疗的中位持续时间为4.6个月中位累积剂量为1230mg。nal-IRI联合5-FU/LV的客观缓解率为2.9%,11例(31.4%)患者病情稳定。在中位随访9.2[95%置信区间(CI):7.8-10.5]个月期间,中位无进展生存期(PFS)和总生存期(OS)分别为2.0(95%CI:1.4-2.6)个月和4.4(95%CI:3.6-5.7)个月。6个月的PFS率和OS率分别为16.3%和37.5%。中位TTPr为0.41(范围0.07-2.07),与先前伊立替康治疗的累积剂量呈负相关(R=-0.3(P=<0.041)。观察到TTPr与先前伊立替康治疗的持续时间之间存在初步负相关(P=-0.35,P=0.062)。最常见的3-4级毒性是中性粒细胞减少(20%)和疲劳(8.6%)。
对于先前接受过含传统伊立替康化疗的mPAC患者,nal-IRI联合5-FU/LV显示出适度的疗效和可管理的毒性。先前传统伊立替康治疗的累积剂量可能与nal-IRI联合5-FU/LV的疗效呈负相关。