Department of Non-Communicable Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Institute of Health Informatics, University College London, London, UK.
Lancet Digit Health. 2021 Dec;3(12):e773-e783. doi: 10.1016/S2589-7500(21)00203-X.
Although acute respiratory infections can lead to cardiovascular complications, the effect of underlying cardiovascular risk on the incidence of acute respiratory infections and cardiovascular complications following acute respiratory infection in individuals without established cardiovascular disease is unknown. We aimed to investigate whether cardiovascular risk is associated with increased risk of acute respiratory infection and acute cardiovascular events after acute respiratory infection using 10 years of linked electronic health record (EHR) data in England.
In this retrospective, population-based cohort study we used EHRs from primary care providers registered on the Clinical Practice Research Datalink (CPRD) GOLD and Aurum databases in England. Eligible individuals were aged 40-64 years, did not have established cardiovascular disease or a chronic health condition that would make them eligible for influenza vaccination, were registered at a general practice contributing to the CPRD, and had linked Hospital Episode Statistics Admitted Patient Care data in England from Sept 1, 2008, to Aug 31, 2018. We classified cardiovascular risk on the basis of diagnosed hypertension and overall predicted cardiovascular risk, estimated by use of the QRISK2 risk-prediction tool (comparing a score of ≥10% [increased risk] with a score of <10% [low risk]). Using multivariable Poisson regression models, we calculated incidence rate ratios (IRRs) for systemic acute respiratory infection. Among individuals who had an acute respiratory infection, we used multivariable Cox regression to calculate hazard ratios (HRs) for the risk of acute cardiovascular events within 1 year of infection.
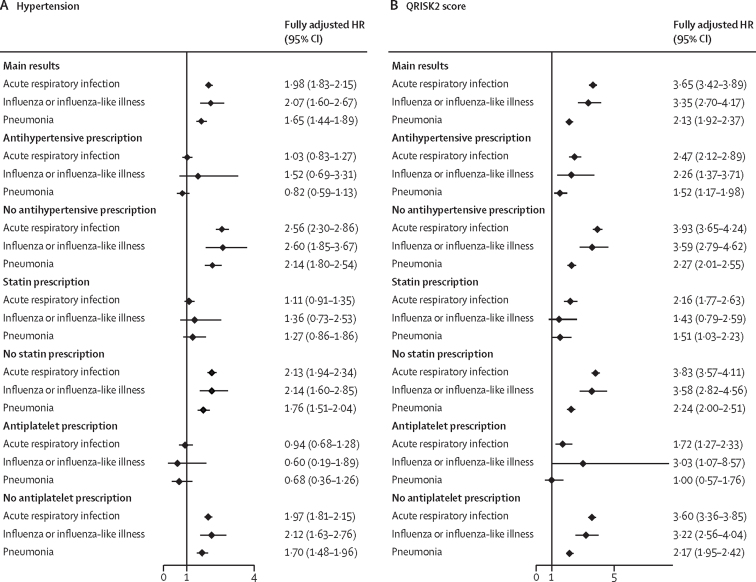
We identified 6 075 321 individuals aged 40-64 years with data in the CPRD and linked data in the Hospital Episode Statistics Admitted Patient Care database between Sept 1, 2008, and Aug 31, 2018. Of these individuals, 4 212 930 (including 526 480 [12·5%] with hypertension and 607 087 [14·4%] with a QRISK2 score of ≥10%) were included in the assessment of the incidence of acute respiratory infection. After adjusting for confounders (age, sex, ethnicity, socioeconomic status, body-mass index, alcohol consumption, smoking status, and consultation frequency in the hypertension analysis; and alcohol consumption and consultation frequency in the QRISK2 analysis), the incidence of acute respiratory infection was higher in individuals with hypertension than those without (IRR 1·04 [95% CI 1·03-1·05]) and higher in those with a QRISK2 score of 10% or higher than in those with a QRISK2 score of less than 10% (1·39 [1·37-1·40]). Of the 442 408 individuals who had an acute respiratory infection, 4196 (0·9%) had an acute cardiovascular event within 1 year of infection. After adjustment (for age, sex, ethnicity, socioeconomic status, body-mass index, alcohol consumption, and smoking status in the hypertension analysis; and for alcohol consumption in the QRISK2 analysis), hypertension (HR 1·98 [95% CI 1·83-2·15]) and a QRISK2 score of 10% or higher (3·65 [3·42-3·89]) were associated with a substantially increased risk of acute cardiovascular events after acute respiratory infection.
People with increased cardiovascular risk but without diagnosed cardiovascular disease, measured by diagnosed hypertension or overall predicted cardiovascular risk, could benefit from influenza and pneumococcal vaccine prioritisation to reduce their risk of both acute respiratory infection and cardiovascular complications following an acute respiratory infection.
British Heart Foundation and the Wellcome Trust.
急性呼吸道感染可导致心血管并发症,但潜在心血管风险对无明确心血管疾病个体急性呼吸道感染后发生急性呼吸道感染和心血管并发症的影响尚不清楚。我们旨在利用英国长达 10 年的电子健康记录(EHR)数据,调查心血管风险是否与急性呼吸道感染后急性呼吸道感染和急性心血管事件的风险增加相关。
在这项回顾性、基于人群的队列研究中,我们使用了英格兰临床实践研究数据链接(CPRD)GOLD 和 Aurum 数据库中初级保健提供者的 EHR。合格个体年龄为 40-64 岁,无明确心血管疾病或慢性健康状况,使其有资格接种流感疫苗,在参加 CPRD 的一般实践中登记,并在英格兰有相关链接的医院入院患者护理数据,时间从 2008 年 9 月 1 日至 2018 年 8 月 31 日。我们根据诊断高血压和使用 QRISK2 风险预测工具(将评分≥10%[风险增加]与评分<10%[低风险]进行比较)估计的总体心血管风险来分类心血管风险。使用多变量泊松回归模型,我们计算了全身急性呼吸道感染的发病率比率(IRR)。在发生急性呼吸道感染的个体中,我们使用多变量 Cox 回归计算了感染后 1 年内发生急性心血管事件的风险比(HR)。
我们确定了 2008 年 9 月 1 日至 2018 年 8 月 31 日期间 CPRD 中有数据且与英格兰医院入院患者护理数据库相关联的 6075321 名年龄在 40-64 岁的个体。其中,4212930 人(包括 526480 人[12.5%]患有高血压和 607087 人[14.4%]的 QRISK2 评分≥10%)被纳入急性呼吸道感染发病率的评估。在调整混杂因素(高血压分析中的年龄、性别、种族、社会经济地位、体重指数、饮酒、吸烟状况和咨询频率;QRISK2 分析中的饮酒和咨询频率)后,高血压患者的急性呼吸道感染发病率高于无高血压患者(IRR 1.04[95%CI 1.03-1.05]),QRISK2 评分≥10%的患者高于 QRISK2 评分<10%的患者(1.39[1.37-1.40])。在 442408 名发生急性呼吸道感染的个体中,4196 名(0.9%)在感染后 1 年内发生急性心血管事件。调整(高血压分析中的年龄、性别、种族、社会经济地位、体重指数、饮酒和吸烟状况;QRISK2 分析中的饮酒状况)后,高血压(HR 1.98[95%CI 1.83-2.15])和 QRISK2 评分≥10%(3.65[3.42-3.89])与急性呼吸道感染后急性心血管事件的风险显著增加相关。
患有增加的心血管风险但没有诊断出心血管疾病的人,通过诊断出的高血压或总体预测的心血管风险来衡量,可以从流感和肺炎球菌疫苗的优先接种中受益,以降低他们在急性呼吸道感染后发生急性呼吸道感染和心血管并发症的风险。
英国心脏基金会和惠康信托基金会。