Liver Diseases-Viral Hepatitis, Liver Unit, Vall d'Hebron Institut de Recerca (VHIR), Vall d'Hebron Hospital Universitari, Vall d'Hebron Barcelona Hospital Campus, Passeig Vall d'Hebron 119-129, 08035 Barcelona, Spain.
Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), Instituto de Salud Carlos III, Av. Monforte de Lemos, 3-5, 28029 Madrid, Spain.
Genes (Basel). 2021 Oct 28;12(11):1731. doi: 10.3390/genes12111731.
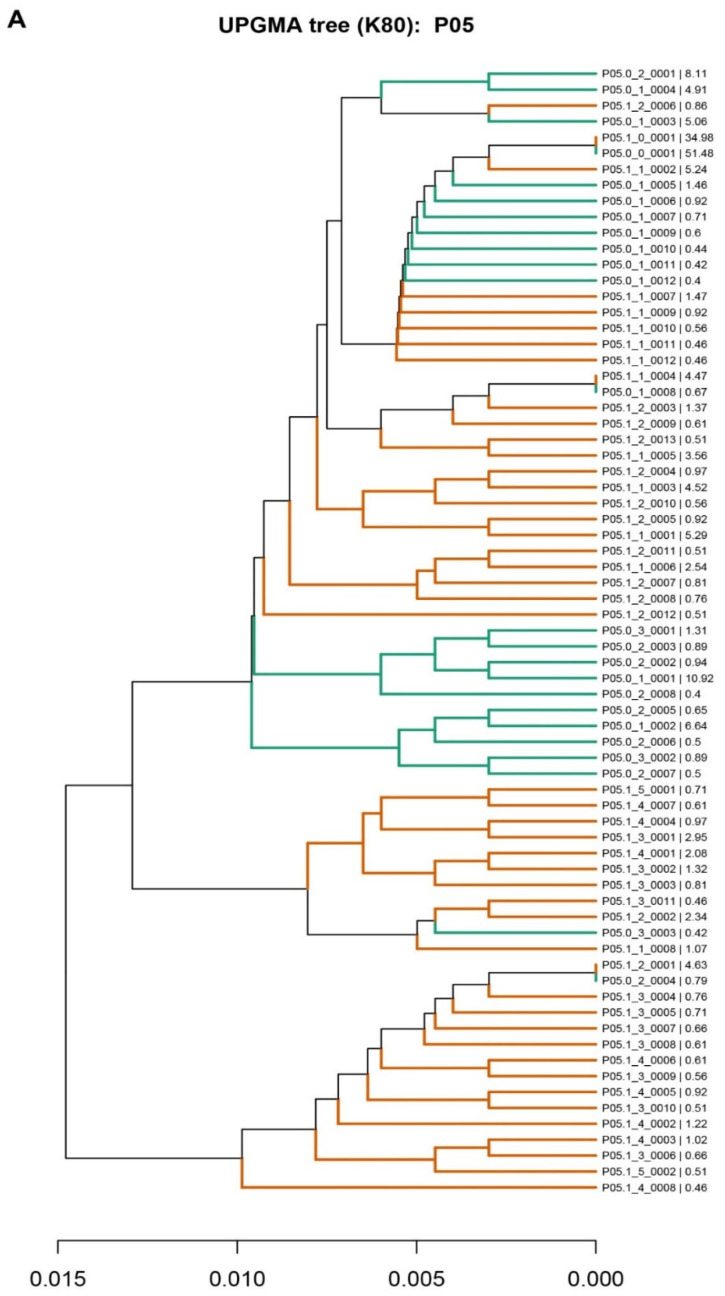
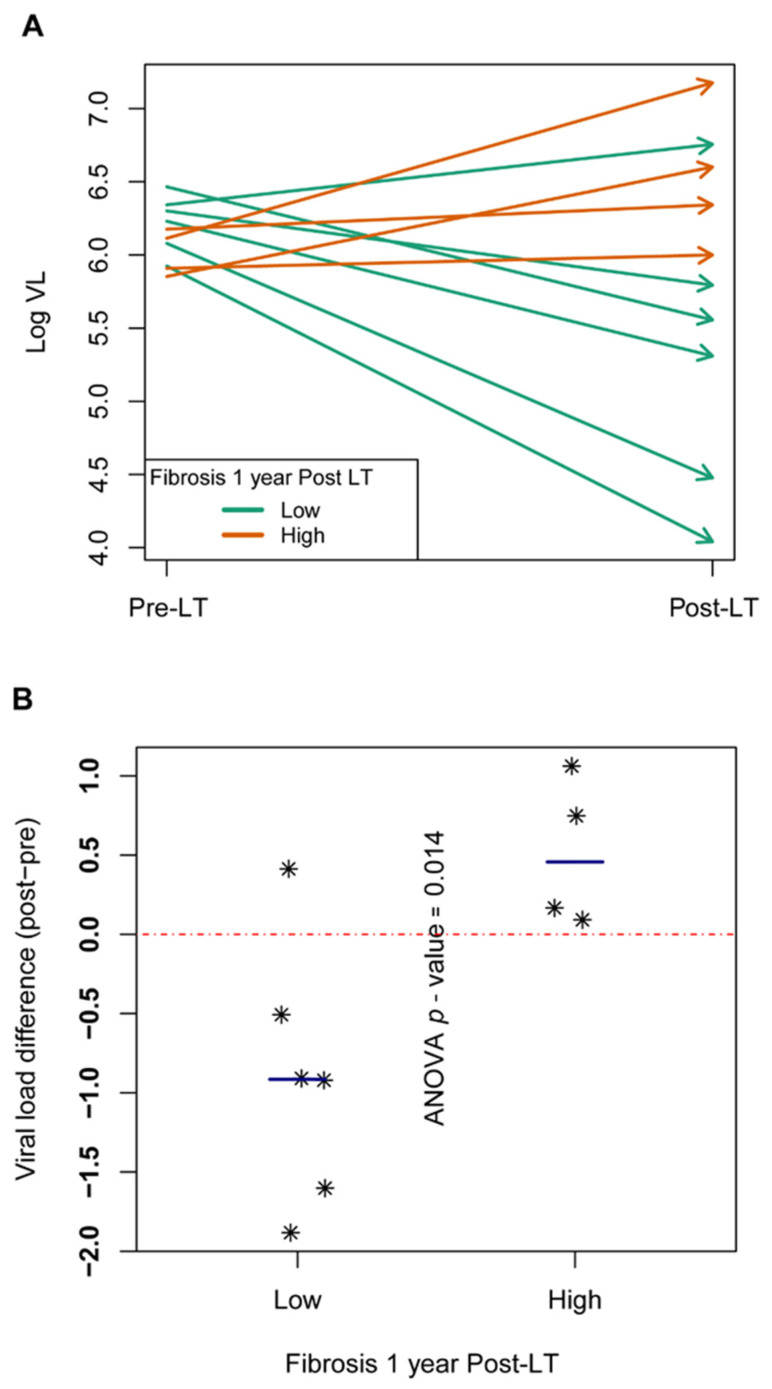
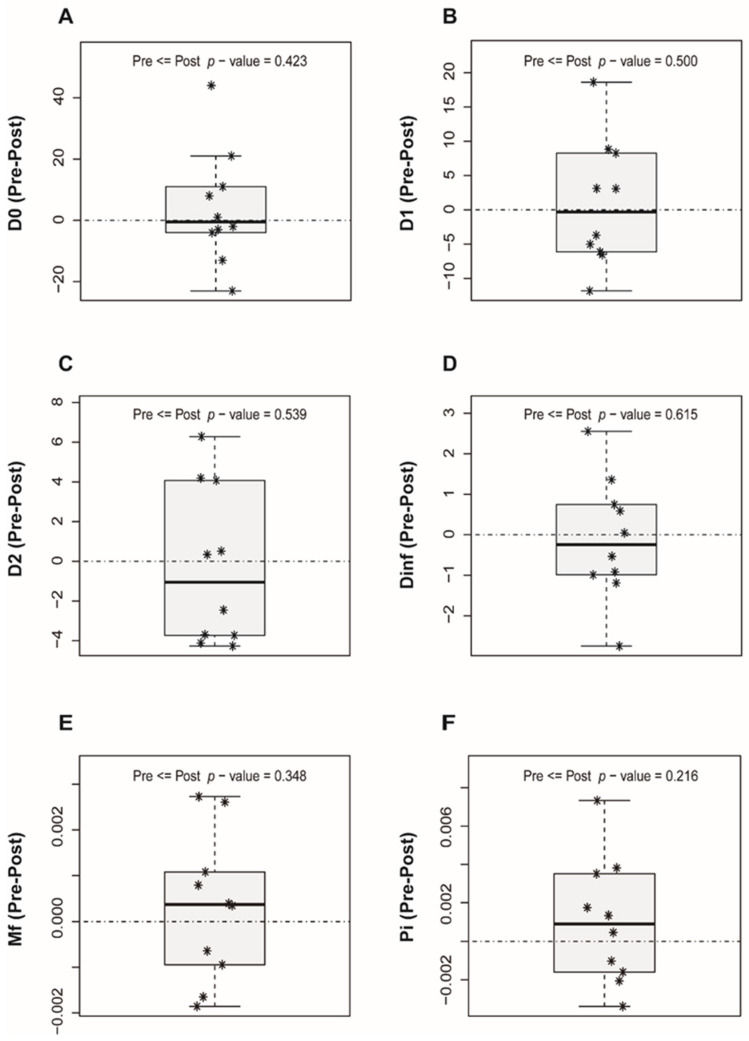
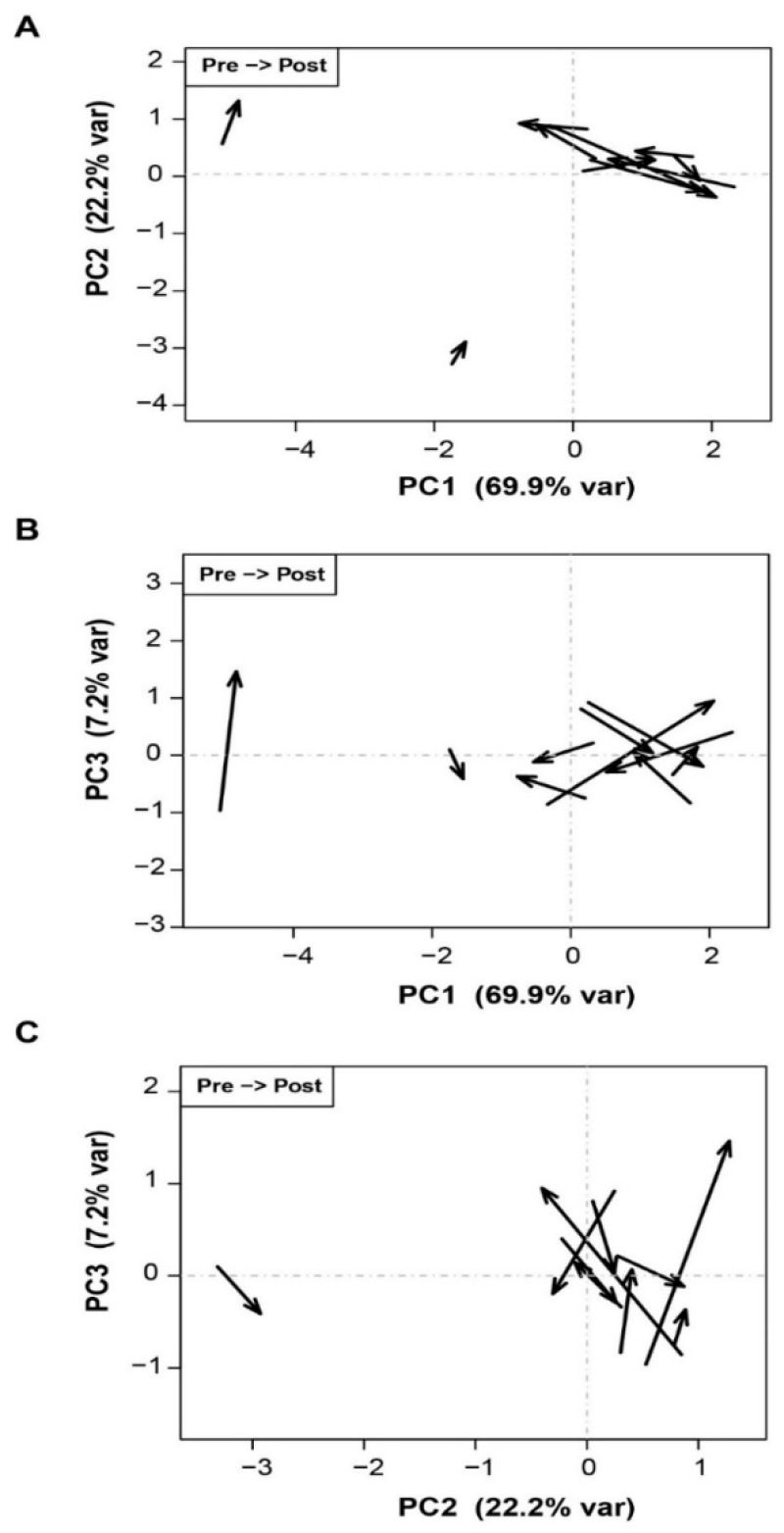
Cirrhosis derived from chronic hepatitis C virus (HCV) infection is still a common indication for liver transplantation (LT). Reinfection of the engrafted liver is universal in patients with detectable viral RNA at the time of transplant and causes fast progression of cirrhosis (within 5 years) in around one-third of these patients. To prevent damage to the liver graft, effective direct-acting antiviral (DAA) therapy is required as soon as possible. However, because of post-LT clinical instability, it is difficult to determine the optimal time to start DAAs with a low risk of complications. Evaluate changes in quasispecies complexity following LT and seek a predictive index of fast liver damage progression to determine the timing of DAA initiation. HCV genomes isolated from pre-LT and 15-day post-LT serum samples of ten patients, who underwent orthotopic LT, were quantified and sequenced using a next-generation sequencing platform. Sequence alignments, phylogenetic trees, quasispecies complexity measures, biostatistics analyses, adjusted R2 values, and analysis of variance (ANOVA) were carried out. Three different patterns of reinfection were observed (viral bottlenecking, conserved pre-LT population, and mixed populations), suggesting that bottlenecking or homogenization of the viral population is not a generalized effect after liver graft reinfection. None of the quasispecies complexity measures predicted the future degree of liver damage. Higher and more uniform viral load (VL) values were observed in all pre-LT samples, but values were more dispersed in post-LT samples. However, VL increased significantly from the pre-LT to 15-day post-LT samples in patients with advanced fibrosis at 1-year post-LT, suggesting that a VL increase on day 15 may be a predictor of fast liver fibrosis progression. HCV kinetics after LT differ between patients and are not fibrosis-dependent. Higher VL at day 15 post-LT versus pre-LT samples may predict fast liver fibrosis progression.
丙型肝炎病毒(HCV)感染导致的肝硬化仍然是肝移植(LT)的常见适应证。在移植时可检测到病毒 RNA 的患者中,移植物的再感染是普遍存在的,这导致其中约三分之一的患者肝硬化快速进展(在 5 年内)。为了防止肝移植物受损,需要尽快进行有效的直接作用抗病毒(DAA)治疗。然而,由于 LT 后的临床不稳定,难以确定以低并发症风险开始 DAA 的最佳时间。评估 LT 后准种复杂性的变化,并寻找快速肝损伤进展的预测指标,以确定 DAA 启动的时间。对 10 例接受原位 LT 的患者的 LT 前和 LT 后 15 天血清样本中的 HCV 基因组进行了定量和测序,使用下一代测序平台。进行了序列比对、系统发育树、准种复杂性测量、生物统计学分析、调整 R2 值和方差分析(ANOVA)。观察到三种不同的再感染模式(病毒瓶颈、预先存在的 LT 种群保守和混合种群),这表明瓶颈或病毒种群的同质化不是肝移植物再感染后的普遍效应。没有一种准种复杂性测量可以预测未来的肝损伤程度。所有 LT 前样本中的病毒载量(VL)值均较高且更均匀,但 LT 后样本中的值更分散。然而,在 1 年后纤维化进展的患者中,从 LT 前到 LT 后 15 天样本的 VL 显著增加,这表明第 15 天 VL 的增加可能是快速肝纤维化进展的预测指标。LT 后 HCV 动力学在患者之间存在差异,与纤维化无关。与 LT 前样本相比,LT 后 15 天的 VL 更高可能预示着快速肝纤维化进展。