Omar Alexander, Winkelmann Marcel, Liodakis Emmanouil, Clausen Jan-Dierk, Graulich Tilman, Omar Mohamed, Krettek Christian, Macke Christian
Trauma Department, Hannover Medical School, 30625 Hannover, Germany.
Bundeswehr Joint Medical Service, 26384 Wilhelmshaven, Germany.
Diagnostics (Basel). 2021 Nov 21;11(11):2156. doi: 10.3390/diagnostics11112156.
Most patients with blunt aortic injuries, who arrive alive in a clinic, suffer from traumatic pseudoaneurysms. Due to modern treatments, the perioperative mortality has significantly decreased. Therefore, it is unclear how exact the prediction of commonly used scoring systems of the outcome is.
We analyzed data on 65 polytraumatized patients with blunt aortic injuries. The following scores were calculated: injury severity score (ISS), new injury severity score (NISS), trauma and injury severity score (TRISS), revised trauma score coded (RTSc) and acute physiology and chronic health evaluation II (APACHE II). Subsequently, their predictive value was evaluated using Spearman´s and Kendall´s correlation analysis, logistic regression and receiver operating characteristics (ROC) curves.
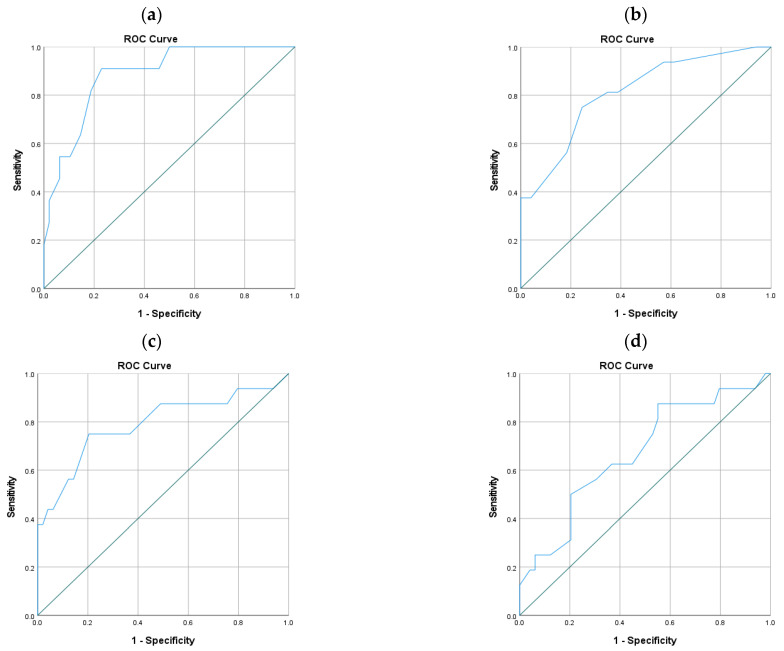
A proportion of 83% of the patients suffered from a thoracic aortic rupture or rupture with concomitant aortic wall dissection (54/65). The overall mortality was 24.6% (16/65). The sensitivity and specificity were calculated as the area under the receiver operating curves (AUC): NISS 0.812, ISS 0.791, APACHE II 0.884, RTSc 0.679 and TRISS 0.761. Logistic regression showed a slightly higher specificity to anatomical scoring systems (ISS 0.959, NISS 0.980, TRISS 0.957, APACHE II 0.938). The sensitivity was highest in the APACHE II with 0.545. Sensitivity and specificity for the RTSc were not significant.
The predictive abilities of all scoring systems were very limited. All scoring systems, except the RTSc, had a high specificity but a low sensitivity. In our study population, the RTSc was not applicable. The APACHE II was the most sensitive score for mortality. Anatomical scoring systems showed a positive correlation with the amount of transfused blood products.
大多数在诊所存活下来的钝性主动脉损伤患者患有创伤性假性动脉瘤。由于现代治疗方法,围手术期死亡率已显著降低。因此,常用评分系统对预后的预测究竟有多准确尚不清楚。
我们分析了65例钝性主动脉损伤多发伤患者的数据。计算了以下评分:损伤严重程度评分(ISS)、新损伤严重程度评分(NISS)、创伤和损伤严重程度评分(TRISS)、修订创伤评分编码(RTSc)和急性生理与慢性健康状况评估II(APACHE II)。随后,使用Spearman和Kendall相关性分析、逻辑回归和受试者工作特征(ROC)曲线评估它们的预测价值。
83%的患者患有胸主动脉破裂或伴有主动脉壁夹层的破裂(54/65)。总死亡率为24.6%(16/65)。敏感性和特异性计算为受试者工作曲线下面积(AUC):NISS为0.812,ISS为0.791,APACHE II为0.884,RTSc为0.679,TRISS为0.761。逻辑回归显示解剖学评分系统的特异性略高(ISS为0.959,NISS为0.980,TRISS为0.957,APACHE II为0.938)。APACHE II的敏感性最高,为0.545。RTSc的敏感性和特异性不显著。
所有评分系统的预测能力都非常有限。除RTSc外,所有评分系统都具有高特异性但低敏感性。在我们的研究人群中,RTSc不适用。APACHE II是对死亡率最敏感的评分。解剖学评分系统与输注血液制品的量呈正相关。