Servei d'Hematologia, Vall d'Hebron Hospital Universitari, Experimental Hematology, Vall d'Hebron Institute of Oncology (VHIO), Vall d'Hebron Barcelona Hospital Campus, Barcelona, Spain.
Department of Medicine, Universitat Autònoma de Barcelona, Bellaterra, Spain.
Blood Adv. 2022 Feb 8;6(3):774-784. doi: 10.1182/bloodadvances.2021006101.
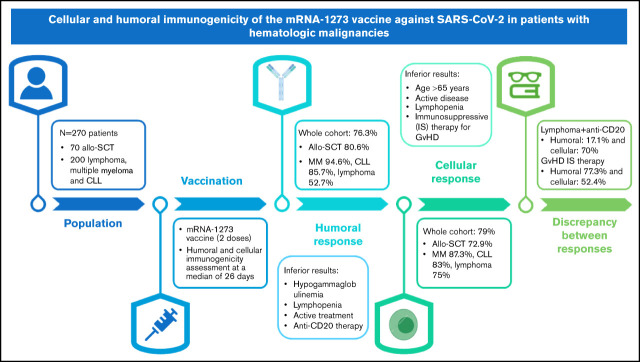
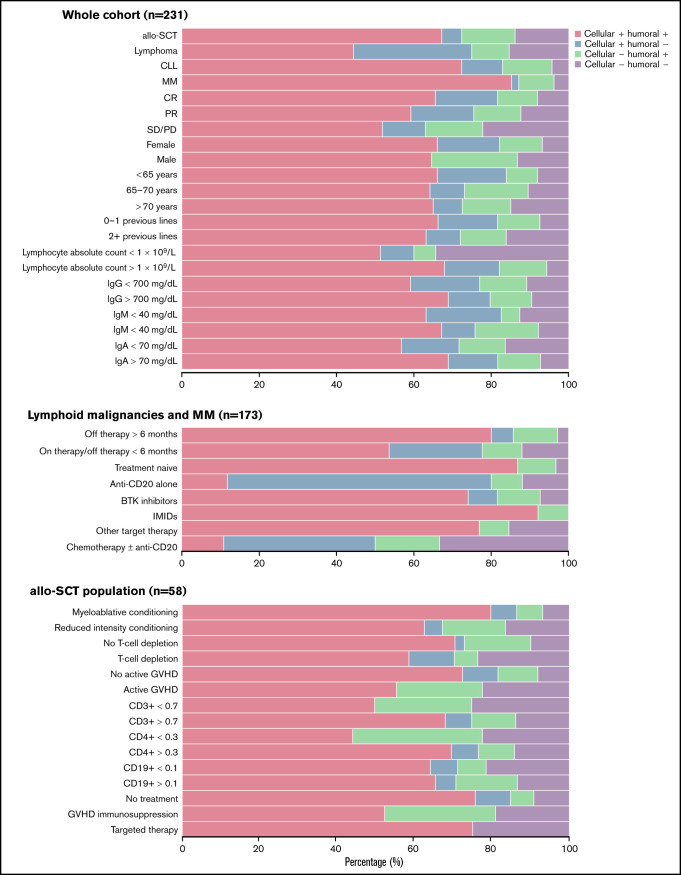
Recent studies have shown a suboptimal humoral response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) messenger RNA (mRNA) vaccines in patients diagnosed with hematologic malignancies; however, data about cellular immunogenicity are scarce. The aim of this study was to evaluate both the humoral and cellular immunogenicity 1 month after the second dose of the mRNA-1273 vaccine. Antibody titers were measured by using the Elecsys and LIAISON anti-SARS-CoV-2 S assays, and T-cell response was assessed by using interferon-γ release immunoassay technology. Overall, 76.3% (184 of 241) of patients developed humoral immunity, and the cellular response rate was 79% (184 of 233). Hypogammaglobulinemia, lymphopenia, active hematologic treatment, and anti-CD20 therapy during the previous 6 months were associated with an inferior humoral response. Conversely, age >65 years, active disease, lymphopenia, and immunosuppressive treatment of graft-versus-host disease (GVHD) were associated with an impaired cellular response. A significant dissociation between the humoral and cellular responses was observed in patients treated with anti-CD20 therapy (the humoral response was 17.5%, whereas the cellular response was 71.1%). In these patients, B-cell aplasia was confirmed while T-cell counts were preserved. In contrast, humoral response was observed in 77.3% of patients undergoing immunosuppressive treatment of GVHD, whereas only 52.4% had a cellular response. The cellular and humoral responses to the SARS-CoV-2 mRNA-1273 vaccine in patients with hematologic malignancies are highly influenced by the presence of treatments such as anti-CD20 therapy and immunosuppressive agents. This observation has implications for the further management of these patients.
最近的研究表明,患有血液恶性肿瘤的患者对严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)信使 RNA(mRNA)疫苗的体液反应不佳;然而,关于细胞免疫原性的数据很少。本研究旨在评估 mRNA-1273 疫苗第二剂接种后 1 个月的体液和细胞免疫原性。通过使用 Elecsys 和 LIAISON 抗 SARS-CoV-2 S 测定法测量抗体滴度,通过干扰素-γ释放免疫测定技术评估 T 细胞反应。总体而言,76.3%(241 例中的 184 例)的患者产生了体液免疫,细胞反应率为 79%(233 例中的 184 例)。在过去 6 个月内发生低丙种球蛋白血症、淋巴细胞减少、正在进行的血液学治疗和抗 CD20 治疗与体液反应不良相关。相反,年龄>65 岁、疾病活动期、淋巴细胞减少和移植物抗宿主病(GVHD)的免疫抑制治疗与细胞反应受损相关。在接受抗 CD20 治疗的患者中观察到体液和细胞反应之间存在显著的分离(体液反应为 17.5%,而细胞反应为 71.1%)。在这些患者中,确认了 B 细胞发育不全,而 T 细胞计数得以保留。相比之下,在接受 GVHD 免疫抑制治疗的患者中有 77.3%观察到体液反应,而只有 52.4%有细胞反应。血液恶性肿瘤患者对 SARS-CoV-2 mRNA-1273 疫苗的体液和细胞反应受到抗 CD20 治疗和免疫抑制药物等治疗的影响很大。这一观察结果对这些患者的进一步治疗具有重要意义。