Kang Mee Joo, Kim Sun-Whe
Department of Surgery, Center for Liver and Pancreato-Biliary Cancer, National Cancer Center, Goyang, Korea.
Ann Hepatobiliary Pancreat Surg. 2021 Nov 30;25(4):451-455. doi: 10.14701/ahbps.2021.25.4.451.
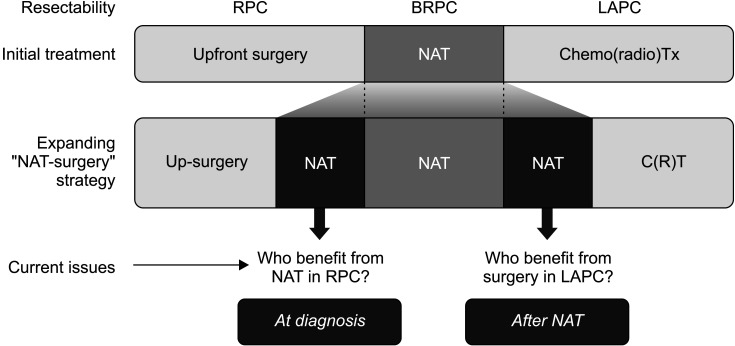
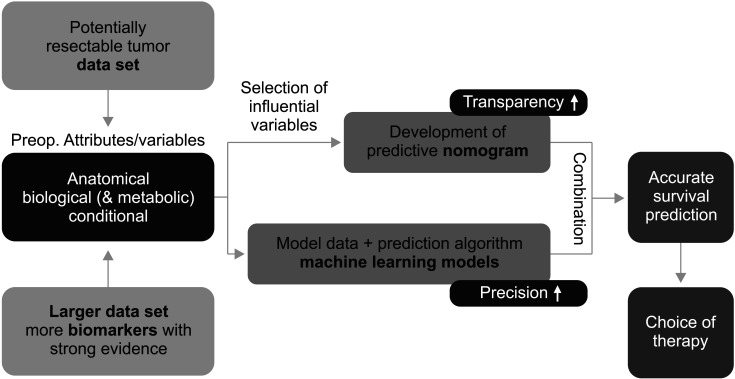
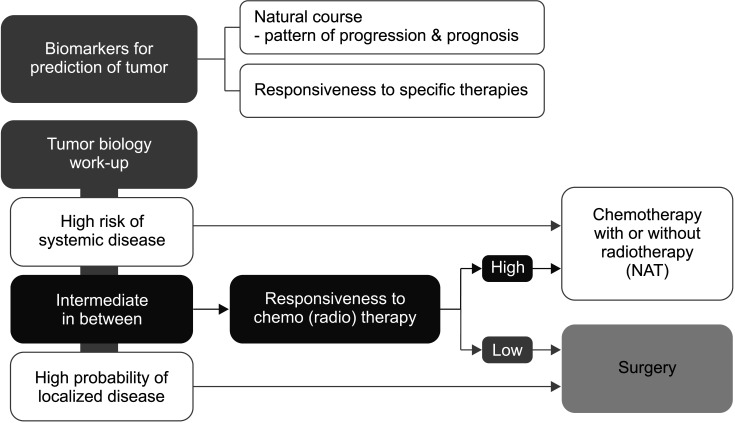
Supported by the expanding indications for neoadjuvant therapy (NAT) for advanced pancreatic cancer (PC), the concept of resectability has evolved from being mostly based on the anatomical tumor extent to considering the biological and conditional factors relevant to prognosis. Therefore, it is more reasonable to define the "criteria for surgical resection" instead of using the "(technical) resectability criteria." NAT has been used in resectable PCs (RPC) with a high risk of early systemic recurrence, as predicted by various biological or anatomical markers. Moreover, the indications for NAT followed by conversion surgery or adjuvant surgery for borderline resectable or locally advanced PC (LAPC) are gradually expanding. Therefore, it is important to define the RPC group that will benefit from NAT and the LAPC group that will benefit from post-NAT surgery. At diagnosis, population-based approaches, such as prognostic stratification and staging systems and personalized outcome-based approaches using prognostic prediction models can be used to determine the criteria for treatment options. Standardized indications for conversion surgery are needed for patients who are initially treated with NAT. In addition to imaging-based morphological criteria, biological criteria, including CA19-9, and various metabolic criteria can be used to establish predicted outcome-based criteria. Multicenter collaboration is required to develop a large database with standardized data collection for various biomarkers and response data after NAT to establish more accurate outcome prediction models to define the new resectability criteria.
在晚期胰腺癌(PC)新辅助治疗(NAT)适应证不断扩大的支持下,可切除性的概念已从主要基于肿瘤的解剖范围演变为考虑与预后相关的生物学和条件因素。因此,定义“手术切除标准”比使用“(技术)可切除性标准”更为合理。NAT已用于具有早期全身复发高风险的可切除性胰腺癌(RPC),这是由各种生物学或解剖学标志物预测的。此外,NAT后进行转化手术或辅助手术治疗临界可切除或局部晚期PC(LAPC)的适应证正在逐渐扩大。因此,确定将从NAT中获益的RPC组和将从NAT后手术中获益的LAPC组非常重要。在诊断时,基于人群的方法,如预后分层和分期系统以及使用预后预测模型的基于个性化结果的方法,可用于确定治疗选择标准。对于最初接受NAT治疗的患者,需要标准化的转化手术适应证。除了基于影像学的形态学标准外,包括CA19-9在内的生物学标准和各种代谢标准可用于建立基于预测结果的标准。需要多中心合作来开发一个大型数据库,对NAT后的各种生物标志物和反应数据进行标准化数据收集,以建立更准确的结果预测模型,从而定义新的可切除性标准。