Non-Communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK
Non-Communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, UK.
BMJ Open. 2021 Nov 30;11(11):e049087. doi: 10.1136/bmjopen-2021-049087.
We aimed to assess the association between multimorbidity and deprivation on short-term mortality among patients with diffuse large B-cell (DLBCL) and follicular lymphoma (FL) in England.
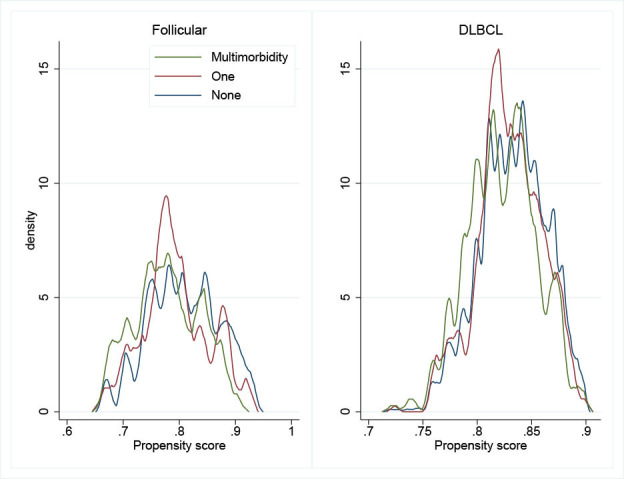
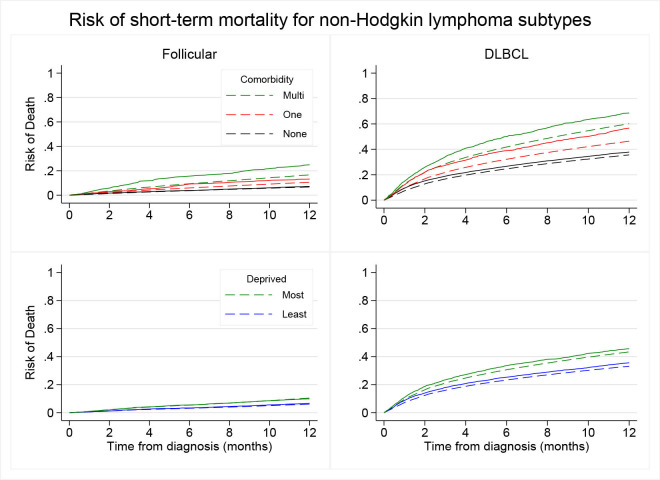
The association of multimorbidity and socioeconomic deprivation on survival among patients diagnosed with DLBCL and FL in England between 2005 and 2013. We linked the English population-based cancer registry with electronic health records databases and estimated adjusted mortality rate ratios by multimorbidity and deprivation status. Using flexible hazard-based regression models, we computed DLBCL and FL standardised mortality risk by deprivation and multimorbidity at 1 year.
Overall, 41 422 patients aged 45-99 years were diagnosed with DLBCL or FL in England during 2005-2015. Most deprived patients with FL with multimorbidities had three times higher hazard of 1-year mortality (HR: 3.3, CI 2.48 to 4.28, p<0.001) than least deprived patients without comorbidity; among DLBCL, there was approximately twice the hazard (HR: 1.9, CI 1.70 to 2.07, p<0.001).
Multimorbidity, deprivation and their combination are strong and independent predictors of an increased short-term mortality risk among patients with DLBCL and FL in England. Public health measures targeting the reduction of multimorbidity among most deprived patients with DLBCL and FL are needed to reduce the short-term mortality gap.
我们旨在评估在英国,弥漫性大 B 细胞淋巴瘤(DLBCL)和滤泡性淋巴瘤(FL)患者中,多种合并症与贫困状况对短期死亡率的关联。
本研究旨在评估 2005 年至 2013 年间,英国诊断为 DLBCL 和 FL 的患者中,多种合并症与社会经济贫困状况对生存的影响。我们将英国人群癌症登记处与电子健康记录数据库相联系,并根据多种合并症和贫困状况评估调整后的死亡率比值。通过灵活的基于危险度的回归模型,我们计算了按贫困和多种合并症分层的 1 年时的 DLBCL 和 FL 标准化死亡率风险。
2005 年至 2015 年间,英格兰共有 41422 名 45-99 岁的患者被诊断为 DLBCL 或 FL。FL 合并多种合并症的最贫困患者在 1 年内死亡的危险度比无合并症的最富裕患者高 3 倍(HR:3.3,95%CI:2.48 至 4.28,p<0.001);在 DLBCL 中,危险度大约增加了两倍(HR:1.9,95%CI:1.70 至 2.07,p<0.001)。
多种合并症、贫困状况及其组合是英格兰 DLBCL 和 FL 患者短期死亡率增加的强有力且独立的预测因素。需要采取公共卫生措施来减少最贫困的 DLBCL 和 FL 患者的多种合并症,以缩小短期死亡率差距。