Pain and Palliative Care Group, School of Health Sciences, Universidad Pontificia Bolivariana, Medellín, Colombia.
Department of Palliative Care, Clínica Cardio VID, Medellín, Colombia.
BMC Palliat Care. 2021 Dec 2;20(1):184. doi: 10.1186/s12904-021-00850-y.
Few hospitals and heart failure (HF) clinics offer concurrent palliative care (PC) together with life-prolonging therapies. To know the prevalence of patients in HF clinics needing PC and useful tools to recognize them are the first steps to extending PC in those settings. However, it is still unknown whether tools commonly used to identify patients with HF needing PC can correctly distinguish them. Two systematic reviews found that the NECesidades PALiativas (NECPAL) tool was one of the two most commonly used tools to asses PC needs in HF patients. Therefore, we assessed 1) the prevalence of PC needs in HF clinics according to the NECPAL tool, and 2) the characteristics of the patients identified as having PC; mainly, their quality of life (QoL), symptom burden, and psychosocial problems.
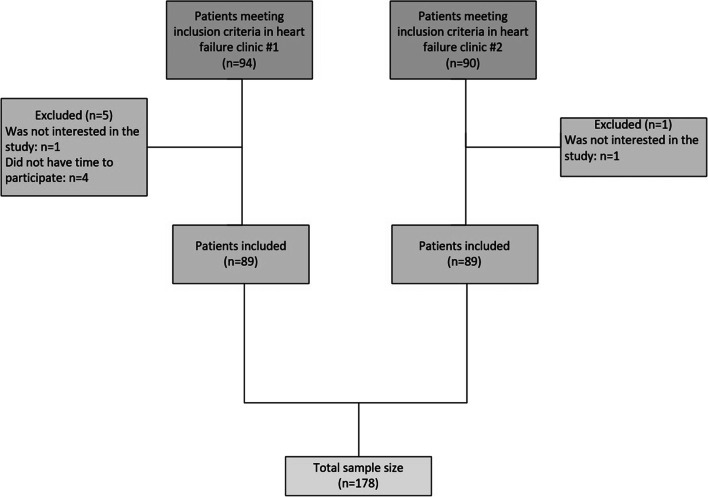
This cross-sectional study was conducted at two HF clinics in Colombia. We assessed the prevalence of PC in the overall sample and in subgroups according to clinical and demographic variables. We assessed QoL, symptom burden, and psychosocial problems using the 12-Item Short-Form Health Survey (SF-12), the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the Edmonton Symptom Assessment System (ESAS). We compared the results of these tools between patients identified as having PC needs (+NECPAL) and patients identified as not having PC needs (-NECPAL).
Among the 178 patients, 78 (44%) had PC needs. The prevalence of PC needs was twice as nigh in patients NYHA III/IV as in patients NYHA I/II and almost twice as high in patients older than 70 years as in patients younger than 70 years. Compared to -NECPAL patients, +NECPAL patients had worse QoL, more severe shortness of breath, tiredness, drowsiness, and pain, and more psychosocial problems.
The prevalence of PC needs in outpatient HF clinics is high and is even higher in older patients and in patients at more advanced NYHA stages. Compared to patients identified as not having PC needs, patients identified as having PC needs have worse QoL, more severe symptoms, and greater psychosocial problems. Including a PC provider in the multidisciplinary team of HF clinics may help to assess and cover these needs.
很少有医院和心力衰竭(HF)诊所同时提供姑息治疗(PC)和延长生命的治疗。了解 HF 诊所中需要 PC 的患者的患病率和识别他们的有用工具是将 PC 扩展到这些环境中的第一步。然而,目前尚不清楚用于识别需要 PC 的 HF 患者的工具是否能够正确地区分他们。两项系统评价发现,NECesidades PALiativas(NECPAL)工具是评估 HF 患者 PC 需求的两种最常用工具之一。因此,我们评估了 1)根据 NECPAL 工具,HF 诊所中 PC 需求的患病率,以及 2)被识别为需要 PC 的患者的特征;主要是他们的生活质量(QoL)、症状负担和心理社会问题。
这项横断面研究在哥伦比亚的两家 HF 诊所进行。我们根据临床和人口统计学变量评估了整体样本和亚组中 PC 的患病率。我们使用 12 项简短健康调查(SF-12)、堪萨斯城心肌病问卷(KCCQ)和埃德蒙顿症状评估系统(ESAS)评估 QoL、症状负担和心理社会问题。我们比较了被识别为有 PC 需求的患者(+NECPAL)和没有 PC 需求的患者(-NECPAL)的这些工具的结果。
在 178 名患者中,有 78 名(44%)有 PC 需求。NYHA III/IV 患者的 PC 需求患病率是 NYHA I/II 患者的两倍,而 70 岁以上患者的 PC 需求患病率几乎是 70 岁以下患者的两倍。与-NECPAL 患者相比,+NECPAL 患者的 QoL 更差,呼吸急促、疲倦、嗜睡和疼痛更严重,心理社会问题更多。
门诊 HF 诊所中 PC 需求的患病率很高,在年龄较大的患者和 NYHA 分期较高的患者中更高。与被识别为没有 PC 需求的患者相比,被识别为有 PC 需求的患者的 QoL 更差,症状更严重,心理社会问题更大。在 HF 诊所的多学科团队中纳入 PC 提供者可能有助于评估和满足这些需求。