Houghton Rebecca, Moore Nathan, Williams Rebecca, El-Bakri Fatima, Peters Jonathan, Mori Matilde, Vernet Gabrielle, Lynch Jessica, Lewis Henry, Tavener Maryanna, Durham Tom, Bowyer Jack, Saeed Kordo, Pollara Gabriele
Hampshire Hospitals NHS Foundation Trust, Hampshire, UK.
University Hospital Southampton NHS Foundation Trust, Southampton, UK.
JAC Antimicrob Resist. 2021 Nov 28;3(4):dlab180. doi: 10.1093/jacamr/dlab180. eCollection 2021 Dec.
A low procalcitonin (PCT) concentration facilitates exclusion of bacterial co-infections in COVID-19, but high costs associated with PCT measurements preclude universal adoption. Changes in inflammatory markers, including C-reactive protein (CRP), can be concordant, and predicting low PCT concentrations may avoid costs of redundant tests and support more cost-effective deployment of this diagnostic biomarker.
To explore whether, in COVID-19, low PCT values could be predicted by the presence of low CRP concentrations.
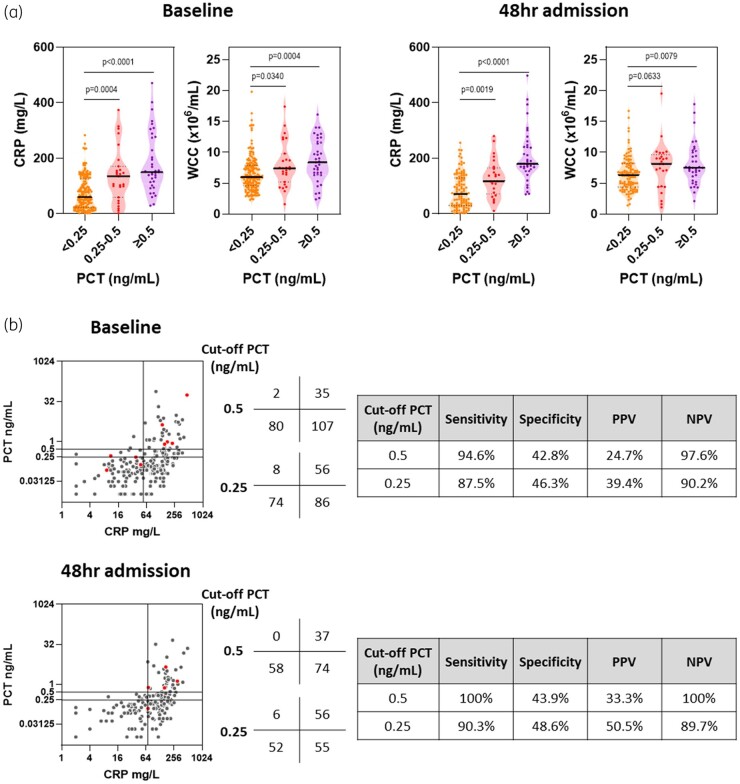
Unselected cohort of 224 COVID-19 patients admitted to hospital that underwent daily PCT and CRP measurements as standard care. Both 0.25 ng/mL and 0.5 ng/mL were used as cut-offs for positive PCT test results. Geometric mean was used to define high and low CRP values at each timepoint assessed.
Admission PCT was <0.25 ng/mL in 160/224 (71.4%), 0.25-0.5 ng/mL in 27 (12.0%) and >0.5 ng/mL in 37 (16.5%). Elevated PCT was associated with increased risk of death (0.0004) and was more commonly associated with microbiological evidence of bacterial co-infection (0.0001). For high CRP values, significant heterogeneity in PCT measurements was observed, with maximal positive predictive value of 50% even for a PCT cut-off of 0.25 ng/mL. In contrast, low CRP was strongly predictive of low PCT concentrations, particularly <0.5 ng/mL, with a negative predictive value of 97.6% at time of hospital admission and 100% 48 hours into hospital stay.
CRP-guided PCT testing algorithms can reduce unnecessary PCT measurement and costs, supporting antimicrobial stewardship strategies in COVID-19.
低降钙素原(PCT)浓度有助于排除新冠病毒病(COVID-19)中的细菌合并感染,但PCT检测成本高昂,阻碍了其普遍应用。包括C反应蛋白(CRP)在内的炎症标志物变化可能一致,预测低PCT浓度可避免重复检测成本,并支持更具成本效益地应用这一诊断生物标志物。
探讨在COVID-19中,低CRP浓度是否可预测低PCT值。
对224例因COVID-19住院的未筛选队列患者进行每日PCT和CRP检测,作为标准护理。PCT检测结果阳性的临界值分别采用0.25 ng/mL和0.5 ng/mL。在每个评估时间点,采用几何平均数来定义CRP的高值和低值。
224例患者中,入院时PCT<0.25 ng/mL的有160例(71.4%),0.25 - 0.5 ng/mL的有27例(12.0%),>0.5 ng/mL的有37例(16.5%)。PCT升高与死亡风险增加相关(0.0004),且更常与细菌合并感染的微生物学证据相关(0.0001)。对于CRP高值,观察到PCT测量存在显著异质性,即使PCT临界值为0.25 ng/mL,最大阳性预测值也仅为50%。相比之下,低CRP强烈预测低PCT浓度,尤其是<0.5 ng/mL,入院时阴性预测值为97.6%,住院48小时后为100%。
CRP指导的PCT检测算法可减少不必要的PCT检测及成本,支持COVID-19中的抗菌管理策略。