Ikezawa Jun, Yokochi Fusako, Okiyama Ryoichi, Kumada Satoko, Tojima Maya, Kamiyama Tsutomu, Hanakawa Takashi, Matsuda Hiroshi, Tanaka Fumiaki, Nakata Yasuhiro, Isozaki Eiji
Department of Neurology, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan.
Department of Neurology and Stroke Medicine, Yokohama City University Graduate School of Medicine, Yokohama, Japan.
Front Neurol. 2021 Nov 18;12:751434. doi: 10.3389/fneur.2021.751434. eCollection 2021.
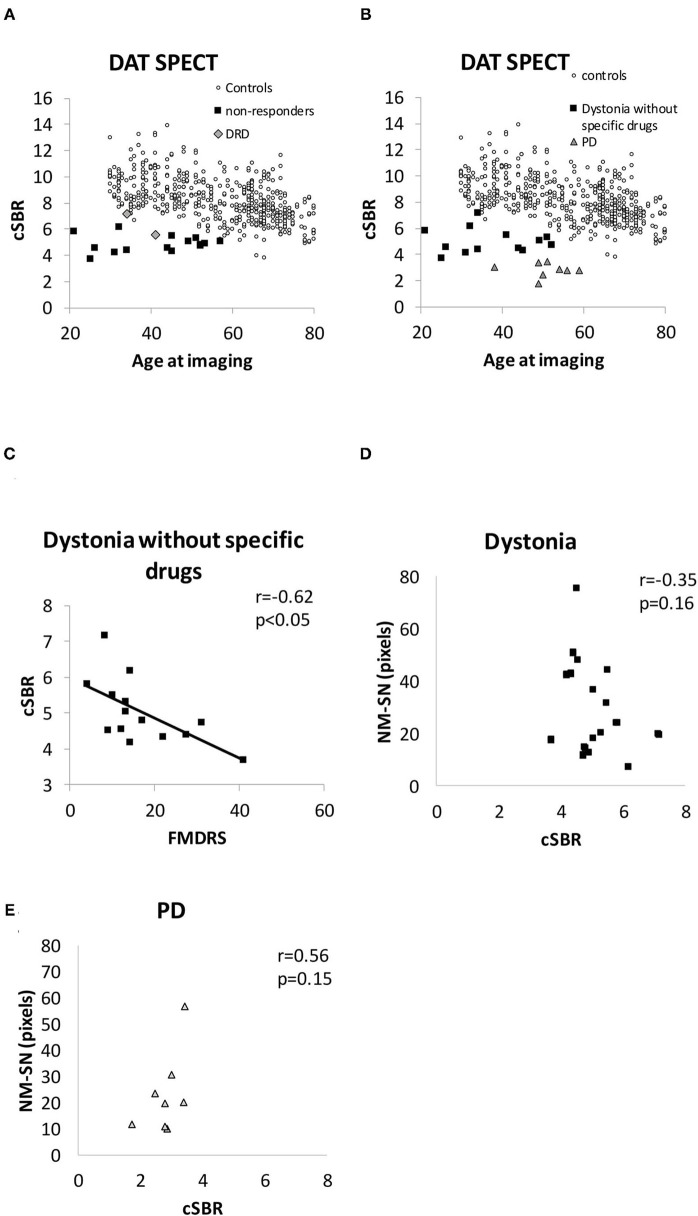
The pathogenesis of dystonia is remarkably diverse. Some types of dystonia, such as DYT5 (DYT-) and tardive dystonia, are related to dysfunction of the dopaminergic system. Furthermore, on pathological examination, cell loss in the substantia nigra (SN) of patients with dystonia has been reported, suggesting that impaired dopamine production may be involved in DYT5 and in other types of dystonia. To investigate functional dopaminergic impairments, we compared patients with dystonia and those with Parkinson's disease (PD) with normal controls using neuromelanin-sensitive magnetic resonance imaging (NM-MRI) and dopamine transporter single photon emission computed tomography (DAT SPECT). A total of 18, 18, and 27 patients with generalized or segmental dystonia, patients with PD, and healthy controls, respectively, were examined using NM-MRI. The mean area corresponding to NM in the SN (NM-SN) was blindly quantified. DAT SPECT was performed on 17 and eight patients with dystonia and PD, respectively. The imaging data of DAT SPECT were harmonized with the Japanese database using striatum phantom calibration. These imaging data were compared between patients with dystonia or PD and controls from the Japanese database in 256 healthy volunteers using the calibrated specific binding ratio (cSBR). The symptoms of dystonia were evaluated using the Fahn-Marsden Dystonia Rating Scale (FMDRS), and the correlation between the results of imaging data and FMDRS was examined. The mean areas corresponding to NM in the SN (NM-SN) were 31 ± 4.2, 28 ± 3.8, and 43 ± 3.8 pixels in patients with dystonia, PD, and in healthy controls, respectively. The mean cSBRs were 5 ± 0.2, 2.8 ± 0.2, 9.2 (predictive) in patients with dystonia, PD, and in healthy controls, respectively. The NM-SN area ( = -0.49, < 0.05) and the cSBR ( = -0.54, < 0.05) were inversely correlated with the FMDRS. There was no significant difference between the dystonia and PD groups regarding NM-SN ( = 0.28). In contrast, the cSBR was lower in patients with PD than in those with dystonia ( < 0.5 × 10). Impairments of the dopaminergic system may be involved in developing generalized and segmental dystonia. SN abnormalities in patients with dystonia were supposed to be different from degeneration in PD.
肌张力障碍的发病机制极为多样。某些类型的肌张力障碍,如DYT5(DYT-)和迟发性肌张力障碍,与多巴胺能系统功能障碍有关。此外,在病理检查中,已有报道称肌张力障碍患者黑质(SN)存在细胞丢失,这表明多巴胺生成受损可能与DYT5及其他类型的肌张力障碍有关。为了研究多巴胺能功能障碍,我们使用神经黑色素敏感磁共振成像(NM-MRI)和多巴胺转运体单光子发射计算机断层扫描(DAT SPECT),将肌张力障碍患者和帕金森病(PD)患者与正常对照进行比较。分别对18例全身性或节段性肌张力障碍患者、18例PD患者和27例健康对照进行了NM-MRI检查。对SN中与神经黑色素对应的平均面积(NM-SN)进行了盲法量化。分别对17例肌张力障碍患者和8例PD患者进行了DAT SPECT检查。使用纹状体模型校准将DAT SPECT的成像数据与日本数据库进行了协调。使用校准后的特异性结合率(cSBR),将肌张力障碍或PD患者与来自日本数据库的256名健康志愿者对照的成像数据进行了比较。使用法恩-马斯登肌张力障碍评定量表(FMDRS)评估肌张力障碍症状,并检查成像数据结果与FMDRS之间的相关性。肌张力障碍患者、PD患者和健康对照中,SN中与神经黑色素对应的平均面积(NM-SN)分别为31±4.2、28±3.8和43±3.8像素。肌张力障碍患者、PD患者和健康对照的平均cSBR分别为5±0.2、2.8±0.2、9.2(预测值)。NM-SN面积(r = -0.49,P < 0.05)和cSBR(r = -0.54,P < 0.05)与FMDRS呈负相关。肌张力障碍组和PD组在NM-SN方面无显著差异(P = 0.28)。相比之下,PD患者的cSBR低于肌张力障碍患者(P < 0.5×10)。多巴胺能系统功能障碍可能参与全身性和节段性肌张力障碍的发生。肌张力障碍患者的SN异常被认为与PD中的变性不同。