Justus Angelo, Burrell Aidan, Anstey Chris, Cornmell George, Brodie Daniel, Shekar Kiran
Adult Intensive Care, Sunshine Coast University Hospital, Sunshine Coast, QLD, Australia.
Australian and New Zealand Intensive Care-Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
Front Med (Lausanne). 2021 Nov 18;8:756280. doi: 10.3389/fmed.2021.756280. eCollection 2021.
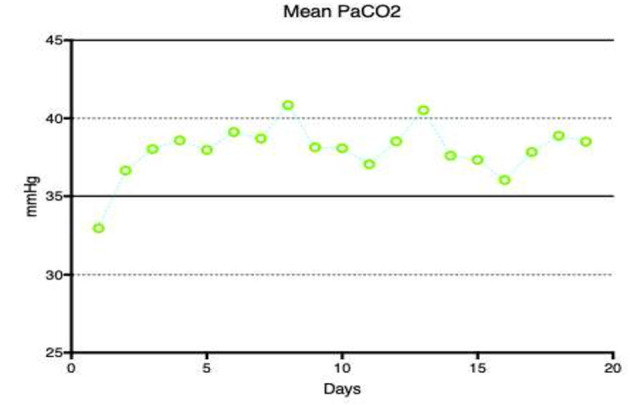
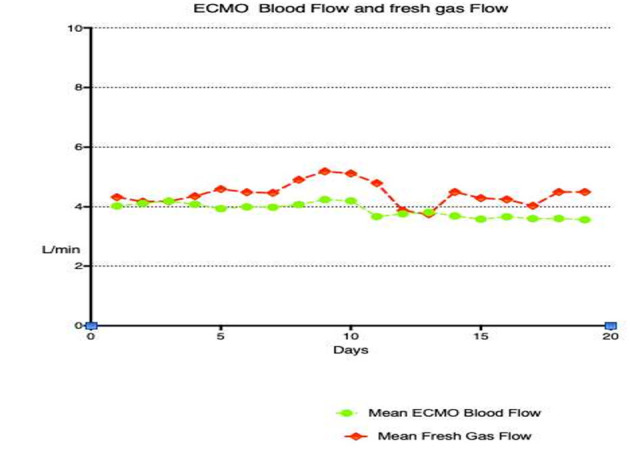
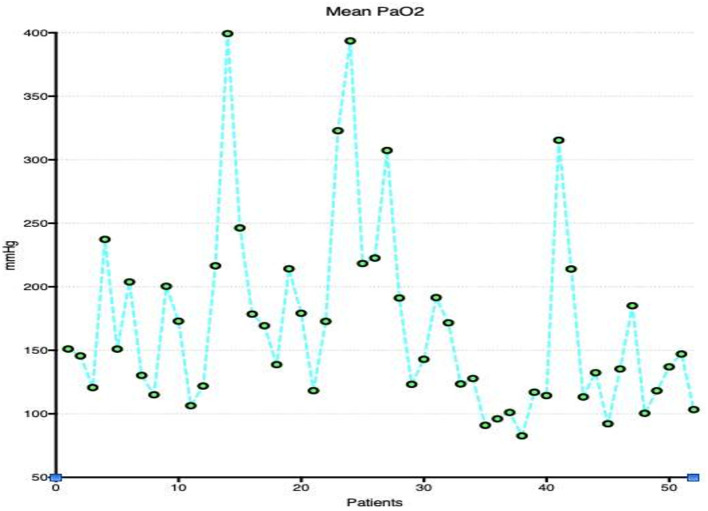
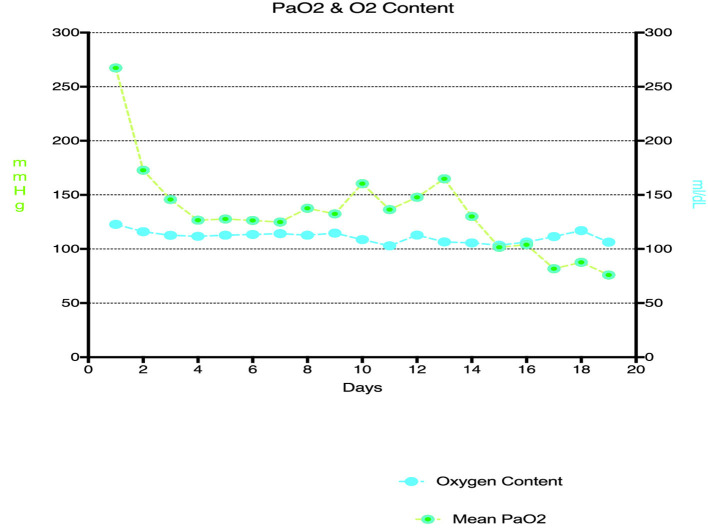
Oxygenation and carbon dioxide removal during venoarterial extracorporeal membrane oxygenation (VA ECMO) depend on a complex interplay of ECMO blood and gas flows, native lung and cardiac function as well as the mechanical ventilation strategy applied. To determine the association of oxygenation, carbon dioxide removal, and mechanical ventilation practices with in-hospital mortality in patients who received VA ECMO. Single center, retrospective cohort study. All consecutive patients who received VA ECMO in a tertiary ECMO referral center over a 5-year period were included. Data on demographics, ECMO and ventilator support details, and blood gas parameters for the duration of ECMO were collected. A multivariable logistic time-series regression model with in-hospital mortality as the primary outcome variable was used to analyse the data with significant factors at the univariate level entered into the multivariable regression model. Overall, 52 patients underwent VA ECMO: 26/52 (50%) survived to hospital discharge. The median PaO for the duration of ECMO support was 146 mmHg [IQR 131-188] and PaCO was 37.2 mmHg [IQR 35.3, 39.9]. Patients who survived to hospital discharge had a significantly lower median PaO (117 [98, 140] vs. 154 [105, 212] mmHg, = 0.04) and higher median PaCO (38.3 [36.1, 41.1] vs. 36.3 [34.5, 37.8] mmHg, = 0.03). Survivors also had significantly lower median VA ECMO blood flow rate (EBFR, 3.6 [3.3, 4.2] vs. 4.3 [3.8, 5.2] L/min, = < 0.001) and greater measured minute ventilation (7.04 [5.63, 8.35] vs. 5.32 [4.43, 6.83] L/min, = 0.01). EBFR, PaO, PaCO, and minute ventilation, however, were not independently associated with death in a multivariable analysis. This exploratory analysis in a small group of VA ECMO supported patients demonstrated that hyperoxemia was common during VA ECMO but was not independently associated with increased mortality. Survivors also received lower EBFR and had greater minute ventilation, but this was also not independently associated with survival. These findings highlight that interactions between EBFR, PaO, and native lung ventilation may be more relevant than their individual association with survival. Further research is indicated to determine the optimal ECMO and ventilator settings on outcomes in VA ECMO.
静脉-动脉体外膜肺氧合(VA ECMO)期间的氧合和二氧化碳清除取决于ECMO血流与气体流量、天然肺和心脏功能以及所采用的机械通气策略之间的复杂相互作用。目的是确定接受VA ECMO治疗的患者的氧合、二氧化碳清除和机械通气实践与院内死亡率之间的关联。这是一项单中心回顾性队列研究。纳入了在一家三级ECMO转诊中心5年期间接受VA ECMO治疗的所有连续患者。收集了患者的人口统计学数据、ECMO和呼吸机支持细节以及ECMO期间的血气参数。以院内死亡率作为主要结局变量的多变量逻辑时间序列回归模型用于分析数据,单变量水平上的显著因素被纳入多变量回归模型。总体而言,52例患者接受了VA ECMO治疗:其中26/52(50%)存活至出院。ECMO支持期间的PaO中位数为146 mmHg[四分位间距(IQR)131 - 188],PaCO中位数为37.2 mmHg[IQR 35.3, 39.9]。存活至出院的患者PaO中位数显著更低(117[98, 140] vs. 154[105, 212] mmHg,P = 0.04),PaCO中位数更高(38.3[36.1, 41.1] vs. 36.3[34.5, 37.8] mmHg,P = 0.03)。存活者的VA ECMO血流量(EBFR)中位数也显著更低(3.6[3.3, 4.2] vs. 4.3[3.8, 5.2] L/min,P = < 0.001),且测得的分钟通气量更大(7.04[5.63, 8.35] vs. 5.32[4.43, 6.83] L/min,P = 0.01)。然而,在多变量分析中,EBFR、PaO、PaCO和分钟通气量与死亡并无独立关联。在一小群接受VA ECMO支持的患者中的这项探索性分析表明,高氧血症在VA ECMO期间很常见,但与死亡率增加并无独立关联。存活者还接受了更低的EBFR且有更大的分钟通气量,但这也与生存并无独立关联。这些发现突出表明,EBFR、PaO和天然肺通气之间的相互作用可能比它们各自与生存的关联更为重要。需要进一步研究以确定VA ECMO中关于结局的最佳ECMO和呼吸机设置。