Service de Réanimation Médicale, centre hospitalier universitaire de Besançon, Besançon, France.
Research Unit EA 3920 and SFR FED 4234, University of Franche Comté, Besancon, France.
Crit Care. 2022 Jul 26;26(1):226. doi: 10.1186/s13054-022-04102-0.
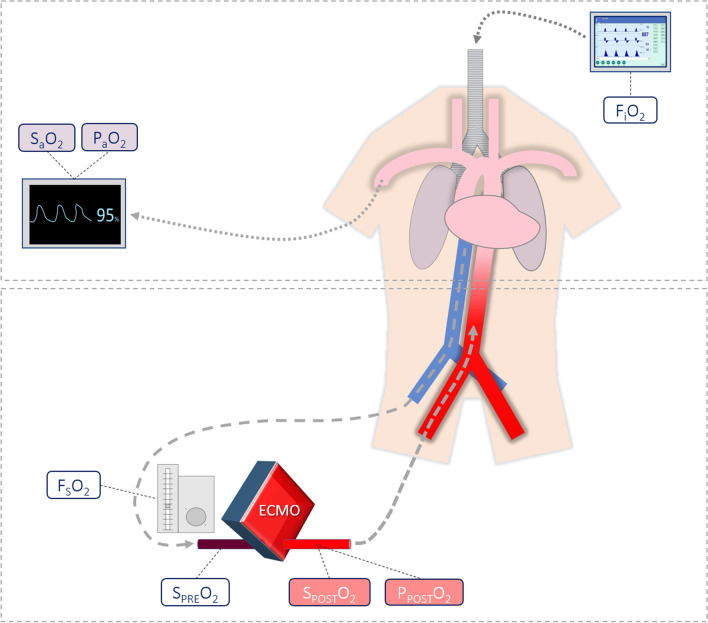
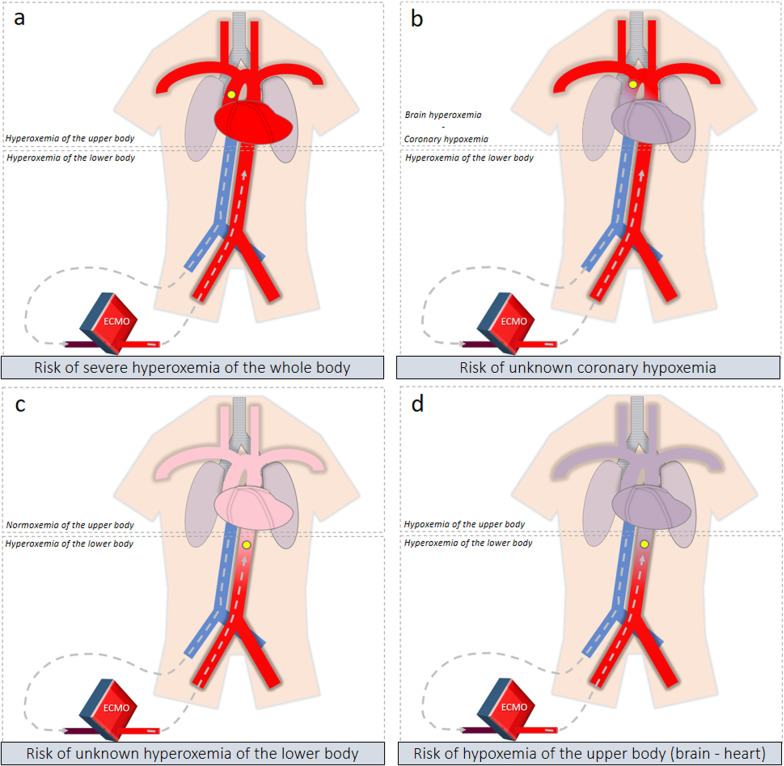
During refractory cardiogenic shock and cardiac arrest, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is used to restore a circulatory output. However, it also impacts significantly arterial oxygenation. Recent guidelines of the Extracorporeal Life Support Organization (ELSO) recommend targeting postoxygenator partial pressure of oxygen (PO) around 150 mmHg. In this narrative review, we intend to summarize the rationale and evidence for this PO target recommendation. Because this is the most used configuration, we focus on peripheral VA-ECMO. To date, clinicians do not know how to set the sweep gas oxygen fraction (FO). Because of the oxygenator's performance, arterial hyperoxemia is common during VA-ECMO support. Interpretation of oxygenation is complex in this setting because of the dual circulation phenomenon, depending on both the native cardiac output and the VA-ECMO blood flow. Such dual circulation results in dual oxygenation, with heterogeneous oxygen partial pressure (PO) along the aorta, and heterogeneous oxygenation between organs, depending on the mixing zone location. Data regarding oxygenation during VA-ECMO are scarce, but several observational studies have reported an association between hyperoxemia and mortality, especially after refractory cardiac arrest. While hyperoxemia should be avoided, there are also more and more studies in non-ECMO patients suggesting the harm of a too restrictive oxygenation strategy. Finally, setting FO to target strict normoxemia is challenging because continuous monitoring of postoxygenator oxygen saturation is not widely available. The threshold of PO around 150 mmHg is supported by limited evidence but aims at respecting a safe margin, avoiding both hypoxemia and severe hyperoxemia.
在难治性心源性休克和心脏骤停期间,使用静脉-动脉体外膜肺氧合(VA-ECMO)来恢复循环输出。然而,它也会显著影响动脉氧合。最近的体外生命支持组织(ELSO)指南建议将氧合器后部分氧分压(PO )目标值设定在 150mmHg 左右。在本叙述性综述中,我们旨在总结该 PO 目标推荐的基本原理和证据。因为这是最常用的配置,所以我们重点关注外周 VA-ECMO。迄今为止,临床医生不知道如何设置吹扫气体氧分数(FO)。由于氧合器的性能,VA-ECMO 支持期间经常会出现动脉高氧血症。在这种情况下,由于双重循环现象,氧合的解释很复杂,这取决于原生心输出量和 VA-ECMO 血流量。这种双重循环导致双重氧合,主动脉内的氧分压(PO)不均匀,器官之间的氧合也不均匀,这取决于混合区的位置。VA-ECMO 期间的氧合数据很少,但有几项观察性研究报告了高氧血症与死亡率之间的关联,尤其是在难治性心脏骤停后。虽然应避免高氧血症,但越来越多的非 ECMO 患者的研究也表明,过于严格的氧合策略也会造成危害。最后,将 FO 设置为目标严格的正常氧合具有挑战性,因为无法广泛获得氧合器后氧饱和度的连续监测。150mmHg 左右的 PO 阈值有有限的证据支持,但旨在尊重安全范围,避免低氧血症和严重高氧血症。