Huang Zhidong, Yang Yanfang, Lu Jin, Liang Jingjing, He Yibo, Yu Yaren, Huang Haozhang, Li Qiang, Wang Bo, Li Shanggang, Yan Zelin, Xu Danyuan, Liu Yong, Chen Kaihong, Huang Zhigang, Ni Jindong, Liu Jin, Chen Liling, Chen Shiqun
Department of Cardiology, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Cardiovascular Institute, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
The Graduate School of Clinical Medicine, Fujian Medical University, Fuzhou, China.
Front Cardiovasc Med. 2021 Nov 17;8:747120. doi: 10.3389/fcvm.2021.747120. eCollection 2021.
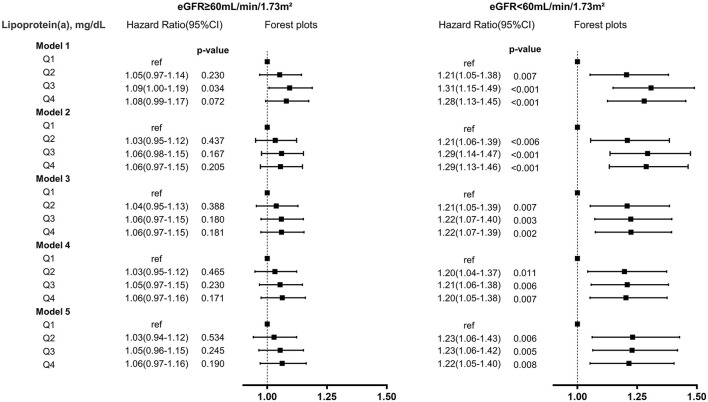
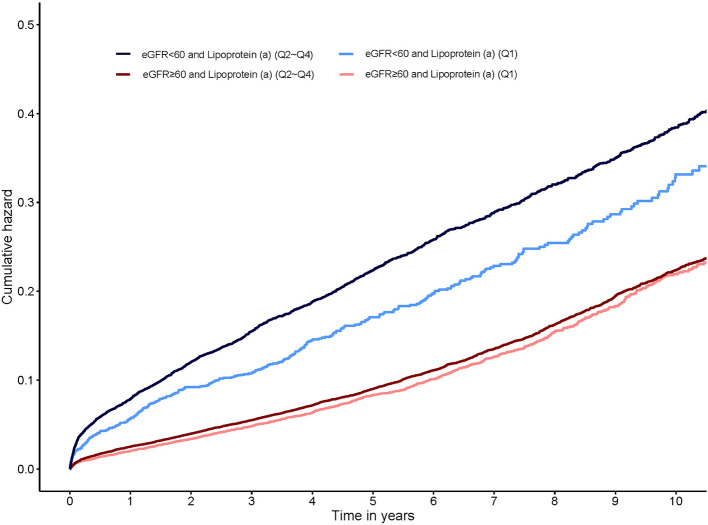
High lipoprotein(a) is associated with poor prognosis in patients at high risk for cardiovascular disease. Renal function based on the estimated glomerular filtration rate (eGFR) is a potential risk factor for the change of lipoprotein(a). However, the regulatory effect of eGFR stratification on lipoprotein(a)-associated mortality has not been adequately addressed. 51,500 patients who underwent coronary angiography (CAG) or percutaneous coronary intervention (PCI) were included from the Cardiorenal ImprovemeNt (CIN) study (ClinicalTrials.gov NCT04407936). These patients were grouped according to lipoprotein(a) quartiles (Q1-Q4) stratified by eGFR categories (<60 and ≥60 mL/min/1.73m). Cox regression models were used to estimate hazard ratios (HR) for mortality across combined eGFR and lipoprotein(a) categories. The mean age of the study population was 62.3 ± 10.6 years, 31.3% were female ( = 16,112). During a median follow-up of 5.0 years (interquartile range: 3.0-7.6 years), 13.0% ( = 6,695) of patients died. Compared with lipoprotein(a) Q1, lipoprotein(a) Q2-Q4 was associated with 10% increased adjusted risk of death in all patients (HR: 1.10 [95% CI: 1.03-1.17]), and was strongly associated with about 23% increased adjusted risk of death in patients with eGFR <60 mL/min/1.73m (HR: 1.23 [95% CI: 1.08-1.39]), while such association was not significant in patients with eGFR ≥60 mL/min/1.73m (HR: 1.05 [95% CI: 0.97-1.13]). P for interaction between lipoprotein(a) (Q1 vs. Q2-Q4) and eGFR (≥60 vs. eGFR <60 mL/min/1.73m) on all-cause mortality was 0.019. Elevated lipoprotein(a) was associated with increased risk of all-cause mortality and such an association was modified by the baseline eGFR in CAG patients. More attention should be paid to the patients with reduced eGFR and elevated lipoprotein(a), and the appropriate lipoprotein(a) intervention is required.
高脂蛋白(a)与心血管疾病高危患者的不良预后相关。基于估算肾小球滤过率(eGFR)的肾功能是脂蛋白(a)变化的一个潜在危险因素。然而,eGFR分层对脂蛋白(a)相关死亡率的调节作用尚未得到充分研究。从心脏肾脏改善(CIN)研究(ClinicalTrials.gov NCT04407936)中纳入了51500例行冠状动脉造影(CAG)或经皮冠状动脉介入治疗(PCI)的患者。这些患者根据按eGFR类别(<60和≥60 mL/min/1.73m²)分层的脂蛋白(a)四分位数(Q1-Q4)进行分组。使用Cox回归模型估计合并eGFR和脂蛋白(a)类别下的死亡风险比(HR)。研究人群的平均年龄为62.3±10.6岁,31.3%为女性(n = 16112)。在中位随访5.0年(四分位间距:3.0-7.6年)期间,13.0%(n = 6695)的患者死亡。与脂蛋白(a) Q1相比,脂蛋白(a) Q2-Q4在所有患者中与调整后死亡风险增加10%相关(HR:1.10 [95%CI:1.03-1.17]),在eGFR<60 mL/min/1.73m²的患者中与调整后死亡风险增加约23%密切相关(HR:1.23 [95%CI:1.08-1.39]),而在eGFR≥60 mL/min/1.73m²的患者中这种关联不显著(HR:1.05 [95%CI:0.97-1.13])。脂蛋白(a)(Q1与Q2-Q4)和eGFR(≥60与eGFR<60 mL/min/1.73m²)对全因死亡率的交互作用P值为0.019。升高的脂蛋白(a)与全因死亡风险增加相关,且这种关联在CAG患者中受基线eGFR的影响。应更多关注eGFR降低且脂蛋白(a)升高的患者,并需要进行适当的脂蛋白(a)干预。