Gerges B, Li W, Leonardi M, Mol B W, Condous G
Acute Gynaecology, Early Pregnancy and Advanced Endosurgery Unit, Sydney Medical School Nepean, University of Sydney, Nepean Hospital, Kingswood, NSW, Australia.
Sydney West Advanced Pelvic Surgery (SWAPS), Blacktown Hospital, Blacktown, NSW, Australia.
Hum Reprod Open. 2021 Nov 4;2021(4):hoab041. doi: 10.1093/hropen/hoab041. eCollection 2021.
Is there an ideal imaging modality for the detection of uterosacral ligaments/torus uterinus (USL), rectovaginal septum (RVS) and vaginal deep endometriosis (DE) in women with a clinical history of endometriosis?
The sensitivity for the detection of USL, RVS and vaginal DE using MRI seems to be better than transvaginal ultrasonography (TVS), whilst the specificity of both were excellent.
The surgical management of women with DE can be complex and requires advanced laparoscopic skills with maximal cytoreduction being vital at the first procedure to provide the greatest symptomatic benefit. Owing to a correlation of TVS findings with surgical findings, preoperative imaging has been used to adequately consent women and plan the appropriate surgery. However, until publication of the consensus statement by the International Deep Endometriosis Analysis Group in 2016, there were significant variations within the terms and definitions used to describe DE in the pelvis.
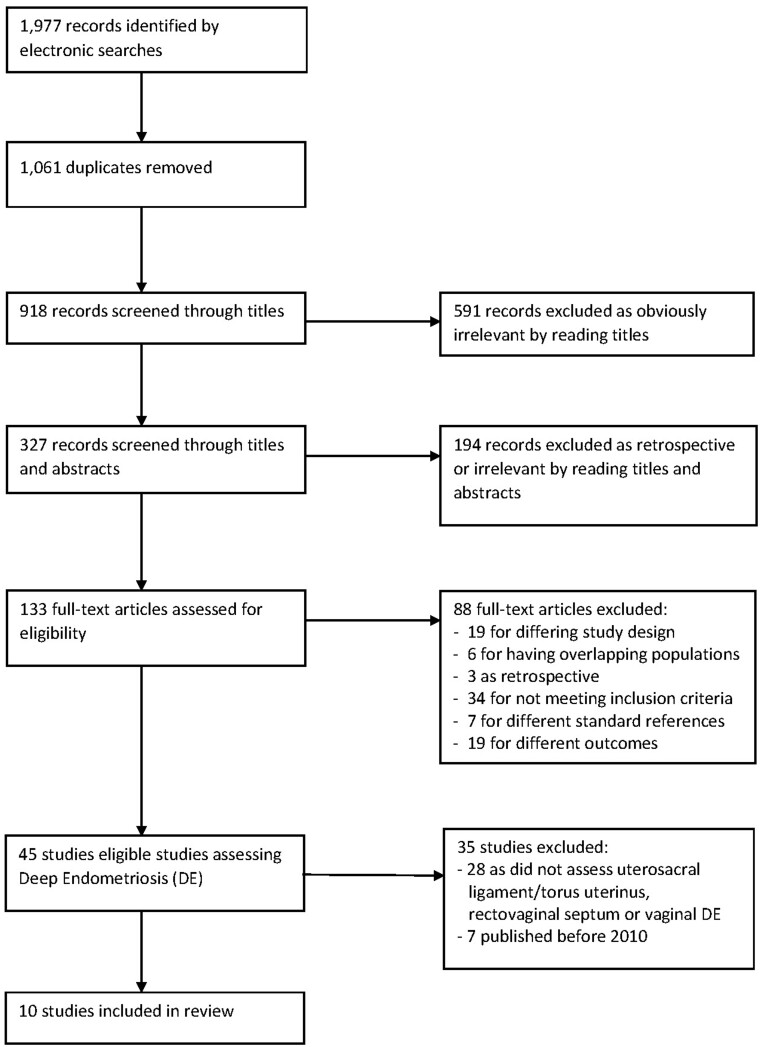
A systematic review and meta-analysis was conducted using Embase, Google Scholar, Medline, PubMed and Scopus to identify studies published from inception to May 2020, of which only those from 2010 were included owing to the increased proficiency of the sonographers and advancements in technology.
PARTICIPANTS/MATERIALS SETTING METHODS: All prospective studies that preoperatively assessed any imaging modality for the detection of DE in the USL, RVS and vagina and correlated with the reference standard of surgical data were considered eligible. Study eligibility was restricted to those including a minimum of 10 unaffected and 10 affected participants.
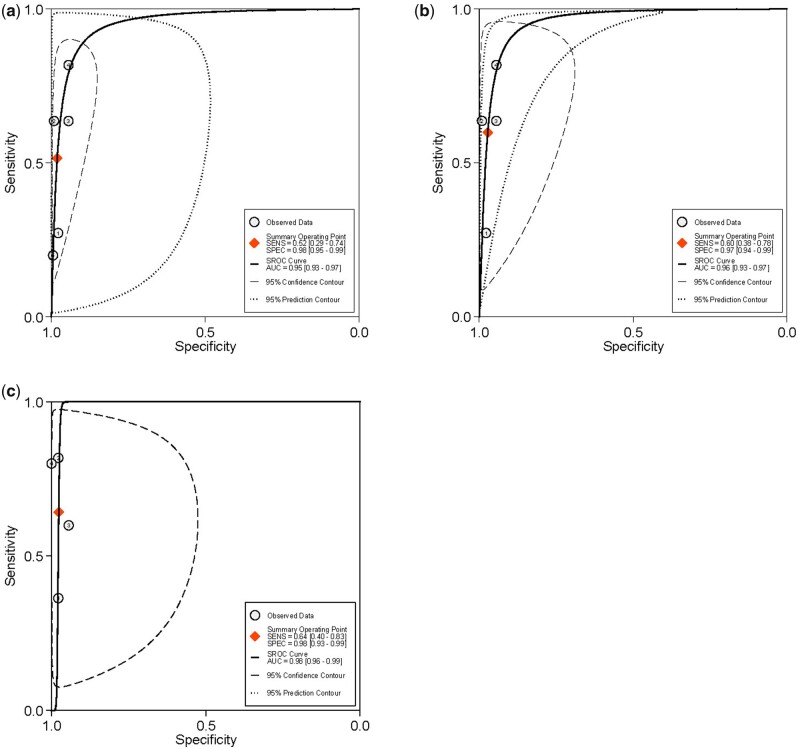
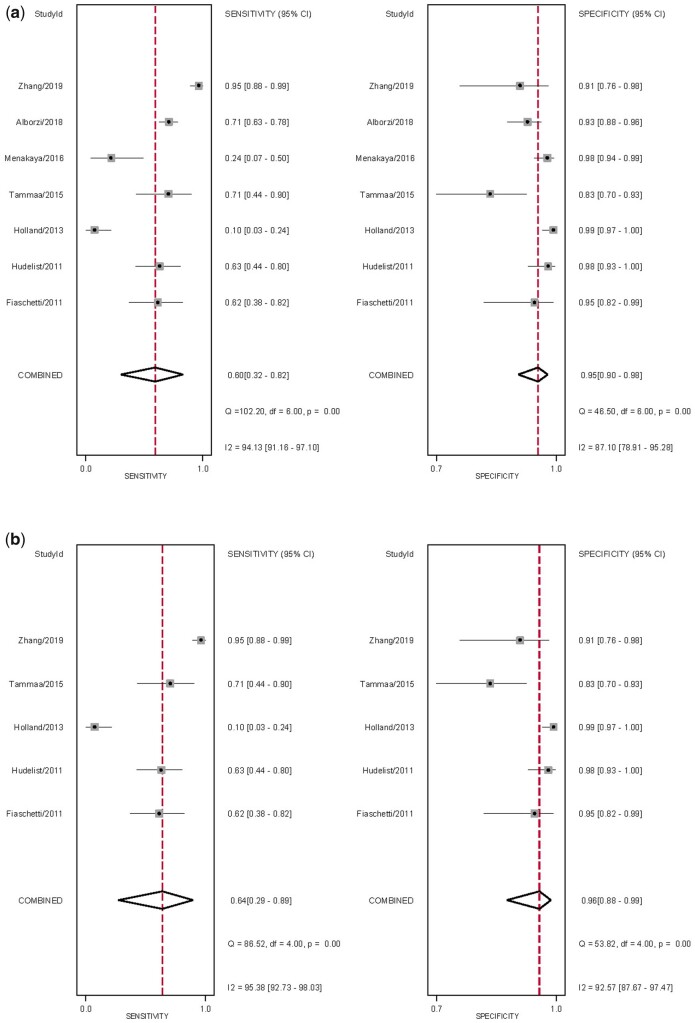
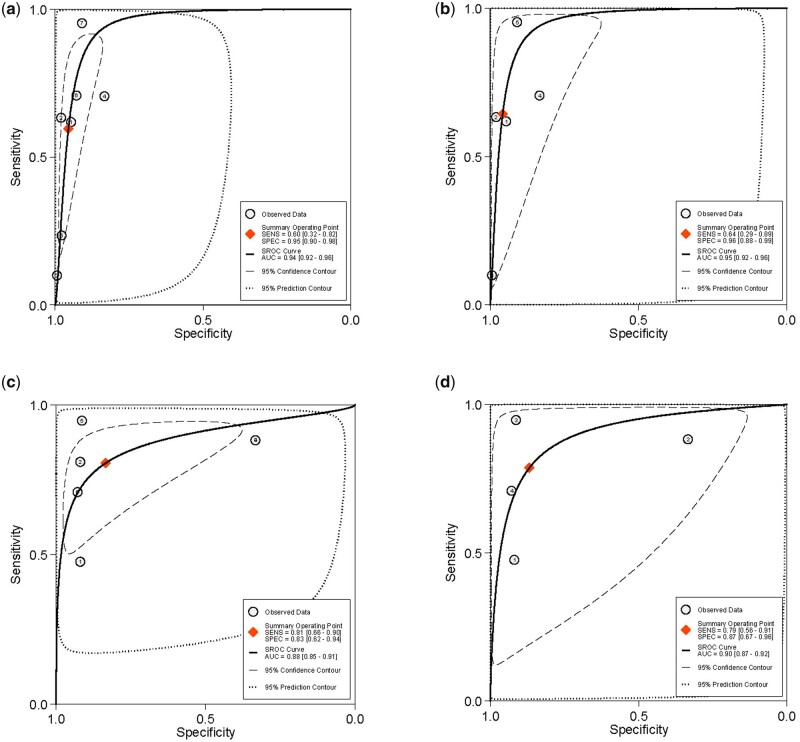
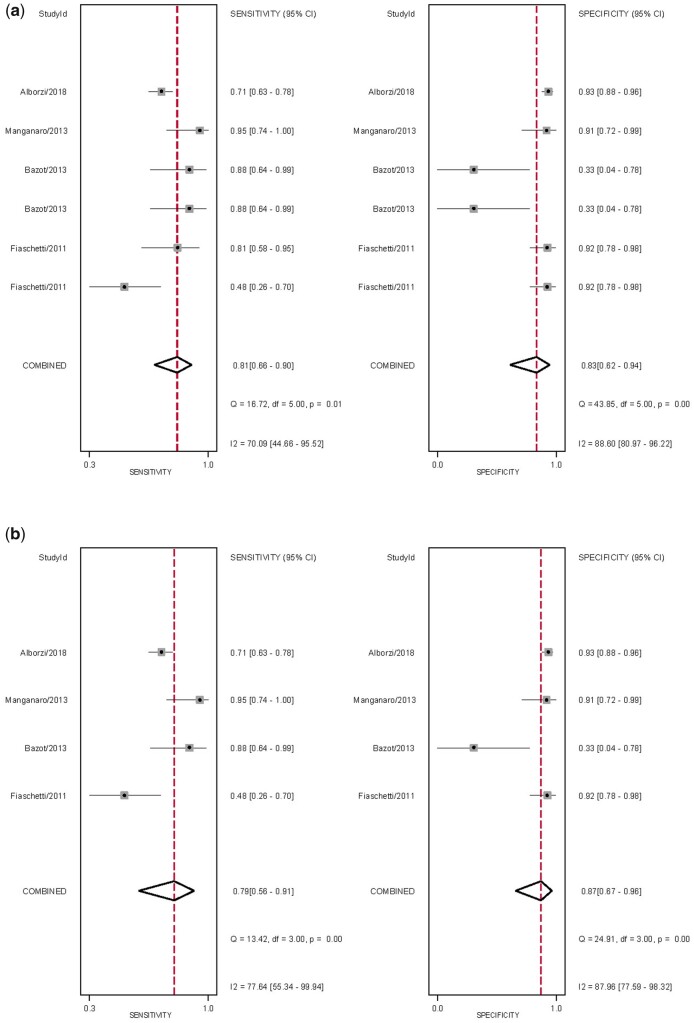
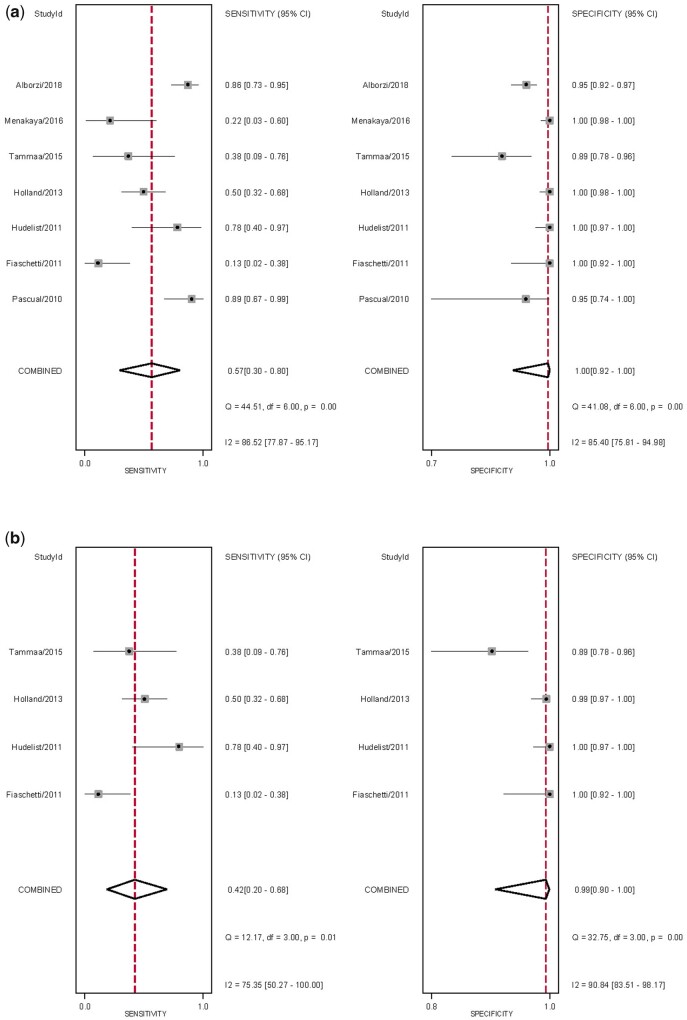
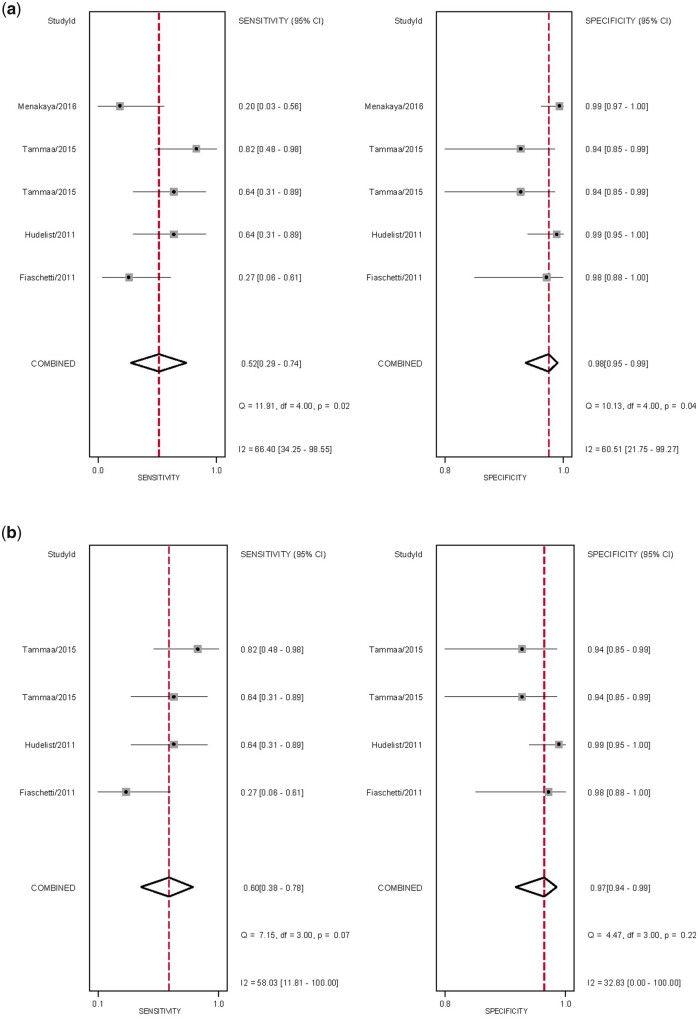
There were 1977 references identified from which 10 studies (n = 1188) were included in the final analysis. For the detection of USL DE, the overall pooled sensitivity and specificity for all TVS techniques were 60% (95% CI 32-82%) and 95% (95% CI 90-98%), respectively, and for all MRI techniques were 81% (95% CI 66-90%) and 83% (95% CI 62-94%), respectively. For the detection of RVS DE, the overall pooled sensitivity and specificity for all TVS techniques were 57% (95% CI 30-80%) and 100% (95% CI 92-100%), respectively. For the detection of vaginal DE, the overall pooled sensitivity and specificity for all TVS techniques were 52% (95% CI 29-74%) and 98% (95% CI 95-99%), respectively, and for all MRI techniques were 64% (95% CI 40-83%) and 98% (96% CI 93-99%). Pooled analyses were not possible for other imaging modalities.
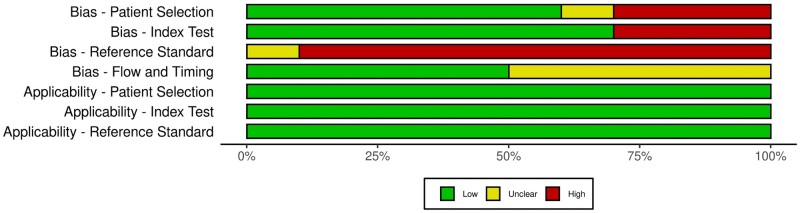
There was a low quality of evidence given the high risk of bias and heterogeneity in the included studies. There are also potential biases secondary to the risk of misdiagnosis at surgery owing to a lack of either histopathological findings or expertise, coupled with the surgeons not being blinded. Furthermore, the varying surgical experience and the lack of clarity regarding complete surgical clearance, thereby also contributing to the lack of histopathology, could also explain the wide range of pre-test probability of disease.
MRI outperformed TVS for the per-operative diagnosis of USL, RVS and vaginal DE with higher sensitivities, although the specificities for both were excellent. There were improved results with other imaging modalities, such as rectal endoscopy-sonography, as well as the addition of bowel preparation or ultrasound gel to either TVS or MRI, although these are based on individual studies.
STUDY FUNDING/COMPETING INTERESTS: No funding was received for this study. M.L. reports personal fees from GE Healthcare, grants from the Australian Women's and Children's Foundation, outside the submitted work. B.W.M. reports grants from NHMRC, outside the submitted work. G.C. reports personal fees from GE Healthcare, outside the submitted work; and is on the Endometriosis Advisory Board for Roche Diagnostics.
Prospective registration with PROSPERO (CRD42017059872) was obtained.
对于有子宫内膜异位症临床病史的女性,是否存在一种理想的成像方式来检测子宫骶韧带/子宫隆凸(USL)、直肠阴道隔(RVS)和阴道深部子宫内膜异位症(DE)?
使用磁共振成像(MRI)检测USL、RVS和阴道DE的敏感性似乎优于经阴道超声检查(TVS),而两者的特异性都很好。
DE女性的手术管理可能很复杂,需要先进的腹腔镜技术,初次手术时最大程度的细胞减灭术对于提供最大的症状改善至关重要。由于TVS检查结果与手术结果相关,术前成像已被用于让女性充分知情并规划合适的手术。然而,在2016年国际深部子宫内膜异位症分析小组发布共识声明之前,用于描述盆腔DE的术语和定义存在很大差异。
研究设计、规模、持续时间:使用Embase、谷歌学术、Medline、PubMed和Scopus进行了一项系统评价和荟萃分析,以识别从开始到2020年5月发表的研究,由于超声检查人员技术水平提高和技术进步,仅纳入了2010年以后的研究。
参与者/材料、环境、方法:所有术前评估任何成像方式以检测USL、RVS和阴道DE并与手术数据参考标准相关的前瞻性研究均被视为合格。研究纳入标准限于至少包括10名未受影响和10名受影响参与者的研究。
共识别出1977篇参考文献,最终分析纳入了10项研究(n = 1188)。对于检测USL DE,所有TVS技术的总体合并敏感性和特异性分别为60%(95%CI 32 - 82%)和95%(95%CI 90 - 98%),所有MRI技术分别为81%(95%CI 66 - 90%)和83%(95%CI 62 - 94%)。对于检测RVS DE,所有TVS技术的总体合并敏感性和特异性分别为57%(95%CI 30 - 80%)和100%(95%CI 92 - 100%)。对于检测阴道DE,所有TVS技术的总体合并敏感性和特异性分别为52%(95%CI 29 - 74%)和98%(95%CI 95 - 99%),所有MRI技术分别为64%(95%CI 40 - 83%)和98%(96%CI 93 - 99%)。其他成像方式无法进行合并分析。
局限性、谨慎的原因:鉴于纳入研究中存在高偏倚风险和异质性,证据质量较低。由于缺乏组织病理学结果或专业知识,手术中存在误诊风险,再加上外科医生未设盲,也存在潜在偏倚。此外,不同的手术经验以及关于完全手术清除的不明确性,进而也导致缺乏组织病理学,这也可以解释疾病的预检概率范围广泛。
MRI在USL、RVS和阴道DE的术中诊断方面优于TVS,敏感性更高,尽管两者的特异性都很好。其他成像方式,如直肠内镜超声检查,以及在TVS或MRI中添加肠道准备或超声凝胶,都有改善结果,尽管这些是基于个别研究。
研究资金/利益冲突:本研究未获得资金。M.L.报告在提交的工作之外从通用电气医疗集团获得个人费用,从澳大利亚妇女和儿童基金会获得资助。B.W.M.报告在提交的工作之外从澳大利亚国家健康与医学研究委员会获得资助。G.C.报告在提交的工作之外从通用电气医疗集团获得个人费用;并在罗氏诊断公司的子宫内膜异位症咨询委员会任职。
已获得PROSPERO(CRD42017059872)的前瞻性注册。