School of Medicine, Yale University, New Haven, CT, USA (Prof A C Justice MD, K S Gordon PhD, E J Edelman MD, J P Tate ScD); VA Connecticut Healthcare System, West Haven, CT, USA (Prof A C Justice, K S Gordon, J P Tate, C T Rentsch PhD, J Womack PhD); Bredesen Center for Interdisciplinary Research and Graduate Education, University of Tennessee, Knoxville, TN, USA (J Romero BSc, P Jones MSc); Biosciences Division, Oak Ridge National Laboratory, Oak Ridge, TN, USA (B J Garcia PhD, D Jacobson PhD); Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, UK (Prof S Khoo MD); Department of Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA (V Lo Re III MD); Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK (C T Rentsch); University Health Network and Faculty of Pharmacy, University of Toronto, Toronto, ON, Canada (A Tseng PharmD); Faculty of Yale University School of Nursing, West Haven, CT, USA (J Womack).
Lancet Healthy Longev. 2021 Oct;2(10):e639-e650. doi: 10.1016/S2666-7568(21)00206-3. Epub 2021 Sep 29.
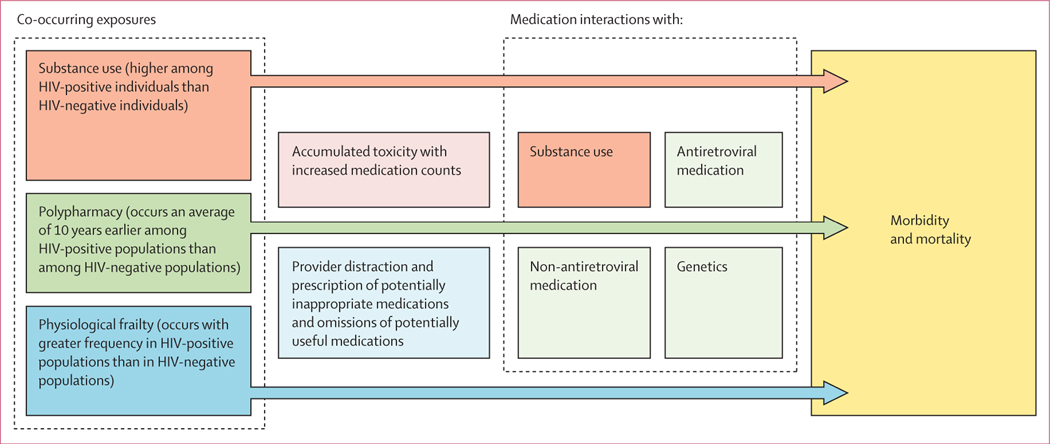
Polypharmacy, defined as use of five or more medications concurrently, is associated with adverse health outcomes and people ageing with HIV might be at greater risk than similar uninfected individuals. We aimed to determine whether known pairwise drug interactions (KPDIs) were associated with risk of admission to hospital (hereafter referred to as hospitalisation) and medication count among people ageing with and without HIV after accounting for physiological frailty.
In this observational study, we collected individual-level data for participants of the Veterans Aging Cohort Study (VACS) with HIV on antiretroviral therapy (ART) and with supressed HIV-1 RNA and people without HIV who were receiving at least one prescription medication, based on active medications in the 2009 fiscal year (ie, Oct 1, 2008, to Sept 30, 2009). We identified KPDIs among these patients by linking prescription fill and refill data with data from DrugBank (version 5.0.11). We collected data on all-cause mortality and hospitalisations between Oct 1, 2009, and March 31, 2019. We compared KPDI counts using random selection and actual patterns of use across medication counts from two to 12. We created a weighted KPDI Index on the basis of the average association of each KPDI with mortality among people ageing without HIV and used nested Cox models stratified by HIV status to estimate the association between medication count and hospitalisation, with incremental adjustments for demographics, physiological frailty, and KPDI Index.
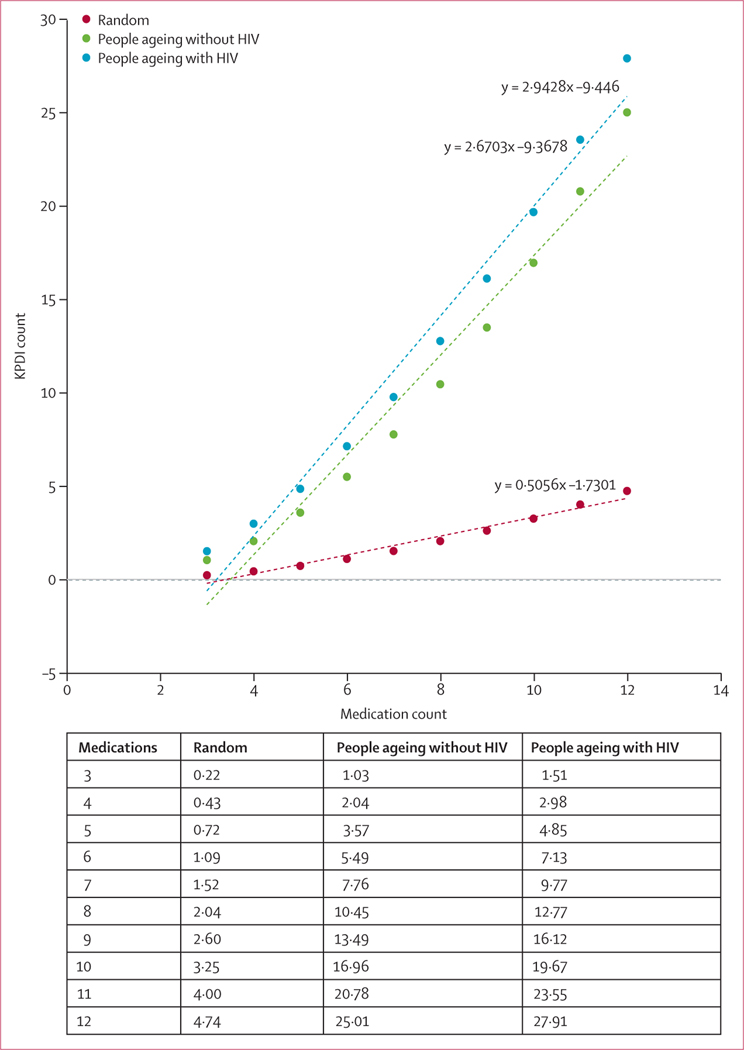
We collected data for 9186 people ageing with HIV and 37 930 individuals without HIV. 45 913 (97·4%) of 47 116 patients were men and the sample was predominantly aged 50-64 years (30 413 [64·6%]). Compared with a random sample of medications, real-world pattern of medication counts and combinations were associated with five-to-six times more KPDIs (eg, for a combination of six medications, KPDI count was 1·09 in the random sample, 5·49 in the HIV-negative population, and 7·13 in the HIV-positive population). For each additional observed medication, people ageing with HIV had approximately 2·94 additional KPDIs and comparators had approximately 2·67 additional KPDIs. Adjustment for demographics, physiological frailty, and KPDI Index reduced the association between medication count and risk of hospitalisation for people ageing with HIV (hazard ratio 1·08 [95% CI 1·07-1·09] reduced to 1·06 [1·05-1·07]) and those without HIV (1·08 [1·07-1·08] reduced to 1·04 [1·03-1·05]).
For each additional medication, people ageing with HIV have more drug-drug interactions than those without HIV. Adjusting for known non-ART drug-drug interactions, each additional non-ART medication confers excess risk of hospitalisation for people ageing with HIV. Randomised trials will be needed to determine whether reducing these interactions improves outcomes.
National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism, Department of Veterans Affairs Health Services Research & Development, and Office of Research and Development.
同时使用五种或以上药物被定义为多重用药,这与不良健康结果相关,而感染 HIV 的老年人比未感染的同龄人面临更大的风险。我们旨在确定已知的药物相互作用(KPDIs)是否与 HIV 感染者和未感染者在考虑生理脆弱性后因住院而入院(以下简称住院)和药物计数相关。
在这项观察性研究中,我们根据 2009 财年(即 2008 年 10 月 1 日至 2009 年 9 月 30 日)的活跃药物,收集了接受抗逆转录病毒治疗(ART)且 HIV-1 RNA 得到抑制的 Veterans Aging Cohort Study(VACS)中的 HIV 感染者和至少服用一种处方药的未感染 HIV 者的个体水平数据。我们通过将处方配药和补充数据与 DrugBank(版本 5.0.11)的数据进行链接,确定了这些患者中的 KPDIs。我们收集了 2009 年 10 月 1 日至 2019 年 3 月 31 日之间的全因死亡率和住院数据。我们比较了 KPDI 计数,随机选择了两种到 12 种药物的计数,并根据 KPDI 与未感染 HIV 者死亡率之间的平均相关性,为 KPDI 指数创建了加权指数。我们使用嵌套 Cox 模型按 HIV 状态分层,根据人口统计学、生理脆弱性和 KPDI 指数进行增量调整,估计了药物计数与住院之间的关联。
我们收集了 9186 名感染 HIV 的老年人和 37930 名未感染 HIV 的个体的数据。47116 名患者中有 45913 名(97.4%)为男性,样本主要年龄在 50-64 岁(30413 名[64.6%])。与随机药物样本相比,实际药物计数和组合与五到六倍的 KPDIs 相关(例如,对于六种药物的组合,随机样本中的 KPDI 计数为 1.09,未感染 HIV 的人群中的 KPDI 计数为 5.49,感染 HIV 的人群中的 KPDI 计数为 7.13)。对于每增加一种观察到的药物,感染 HIV 的老年人大约会增加 2.94 种 KPDIs,而对照组大约会增加 2.67 种 KPDIs。调整人口统计学、生理脆弱性和 KPDI 指数后,感染 HIV 的老年人(风险比 1.08 [95%CI 1.07-1.09]降至 1.06 [1.05-1.07])和未感染 HIV 的老年人(1.08 [1.07-1.08]降至 1.04 [1.03-1.05])与住院风险之间的关联减弱。
对于每增加一种药物,感染 HIV 的老年人比未感染 HIV 的老年人发生药物相互作用的可能性更大。调整已知的非 ART 药物相互作用后,每增加一种非 ART 药物会增加感染 HIV 的老年人住院的风险。需要进行随机试验来确定减少这些相互作用是否能改善结果。
美国国立卫生研究院、国家酒精滥用和酒精中毒研究所、退伍军人事务部卫生服务研究与发展部以及研究与发展办公室。