State Department of Cardiology, Hippokrateion General Hospital, Athens, Greece.
First Department of Cardiology, Hippokrateion General Hospital, National and Kapodistrian University of Athens School of Medicine, Athens, Greece.
Ann Noninvasive Electrocardiol. 2022 Mar;27(2):e12908. doi: 10.1111/anec.12908. Epub 2021 Dec 6.
In the PRESERVE-EF study, a two-step sudden cardiac death (SCD) risk stratification approach to detect post-myocardial infarction (MI) patients with left ventricle ejection fraction (LVEF) ≥40% at risk for major arrhythmic events (MAEs) was used. Seven noninvasive risk factors (NIRFs) were extracted from a 24-h ambulatory electrocardiography (AECG) and a 45-min resting recording. Patients with at least one NIRF present were referred for invasive programmed ventricular stimulation (PVS) and inducible patients received an Implantable Cardioverter - Defibrillator (ICD).
In the present study, we evaluated the performance of the NIRFs, as they were described in the PRESERVE-EF study protocol, in predicting a positive PVS. In the PRESERVE-EF study, 152 out of 575 patients underwent PVS and 41 of them were inducible. For the present analysis, data from these 152 patients were analyzed.
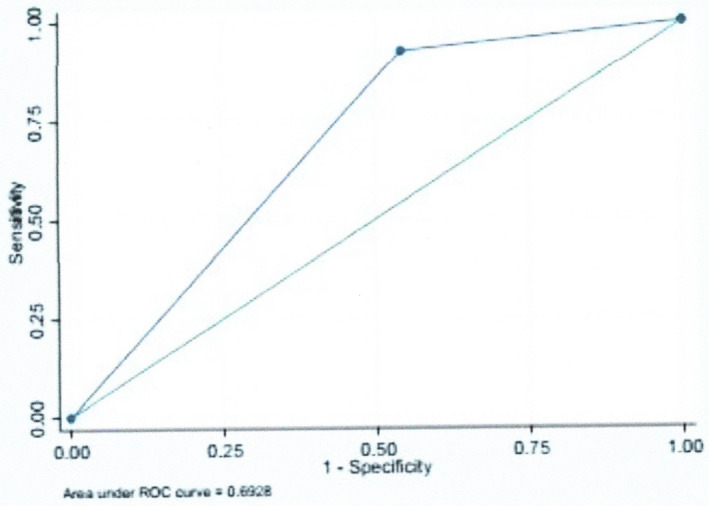
Among the NIRFs examined, the presence of signal averaged ECG-late potentials (SAECG-LPs) ≥ 2/3 and non-sustained ventricular tachycardia (NSVT) ≥1 eposode/24 h cutoff points were important predictors of a positive PVS study, demonstrating in the logistic regression analysis odds ratios 2.285 (p = .027) and 2.867 (p = .006), respectively. A simple risk score based on the above cutoff points in combination with LVEF < 50% presented high sensitivity but low specificity for a positive PVS.
Cutoff points of NSVT ≥ 1 episode/24 h and SAECG-LPs ≥ 2/3 in combination with a LVEF < 50% were important predictors of inducibility. However, the final decision for an ICD implantation should be based on a positive PVS, which is irreplaceable in risk stratification.
在 PRESERVE-EF 研究中,采用两步骤的方法对心肌梗死后左心室射血分数(LVEF)≥40%的患者进行心源性猝死(SCD)风险分层,以检测主要心律失常事件(MAE)的高危患者。从 24 小时动态心电图(AECG)和 45 分钟静息记录中提取了 7 个非侵入性风险因素(NIRFs)。至少存在一个 NIRF 的患者将接受有创程控心室刺激(PVS),可诱导的患者将植入植入式心脏复律除颤器(ICD)。
本研究评估了 PRESERVE-EF 研究方案中描述的 NIRFs 在预测 PVS 阳性方面的性能。在 PRESERVE-EF 研究中,575 例患者中有 152 例接受了 PVS,其中 41 例为可诱导的。本分析中,分析了这 152 例患者的数据。
在检查的 NIRFs 中,信号平均心电图晚期电位(SAECG-LPs)≥2/3 和非持续性室性心动过速(NSVT)≥1 个/24 小时切点是 PVS 阳性的重要预测因素,在逻辑回归分析中,优势比分别为 2.285(p=0.027)和 2.867(p=0.006)。基于上述切点的简单风险评分结合 LVEF<50%,对 PVS 阳性具有高敏感性但特异性低。
NSVT≥1 个/24 小时和 SAECG-LPs≥2/3 切点与 LVEF<50%结合,是可诱导性的重要预测因素。然而,ICD 植入的最终决定应基于 PVS 阳性,这在风险分层中是不可替代的。