Department of Respiratory Medicine, Countess of Chester Hospital NHS Trust, Liverpool Road, Chester, CH2 1UL, UK.
University of Chester Medical School, Chester, UK.
BMC Pulm Med. 2021 Dec 11;21(1):411. doi: 10.1186/s12890-021-01783-1.
Research questions To compare the efficacy of nintedanib and pirfenidone in the treatment of progressive pulmonary fibrosis; and to compare the efficacy of anti-fibrotic therapy (grouping nintedanib and pirfenidone together) in patients with IPF versus patients with progressive lung fibrosis not classified as IPF.
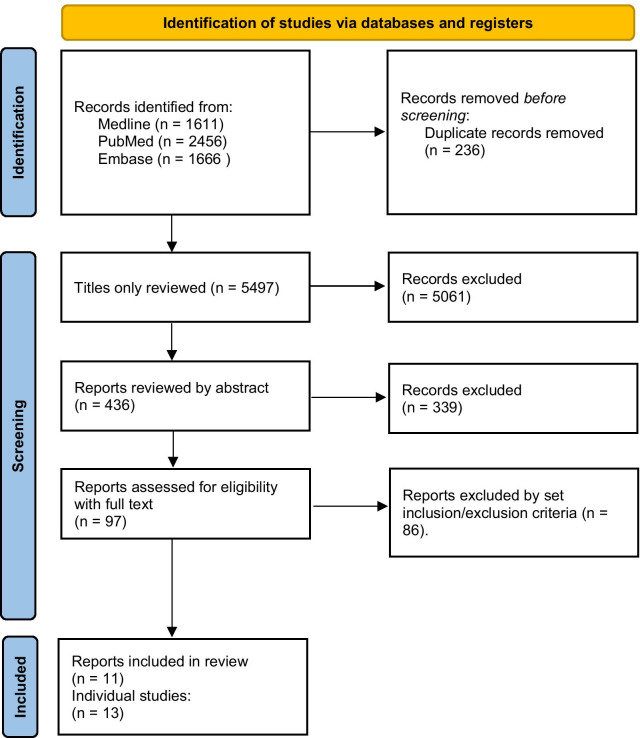
A search of databases including MEDLINE, EMBASE, PubMed, and clinicaltrials.gov was conducted. Studies were included if they were randomised controlled trials of pirfenidone or nintedanib in adult patients with IPF or non-IPF patients, and with extractable data on mortality or decline in forced vital capacity (FVC). Random effects meta-analyses were performed on changes in FVC and where possible on mortality in the selected studies.
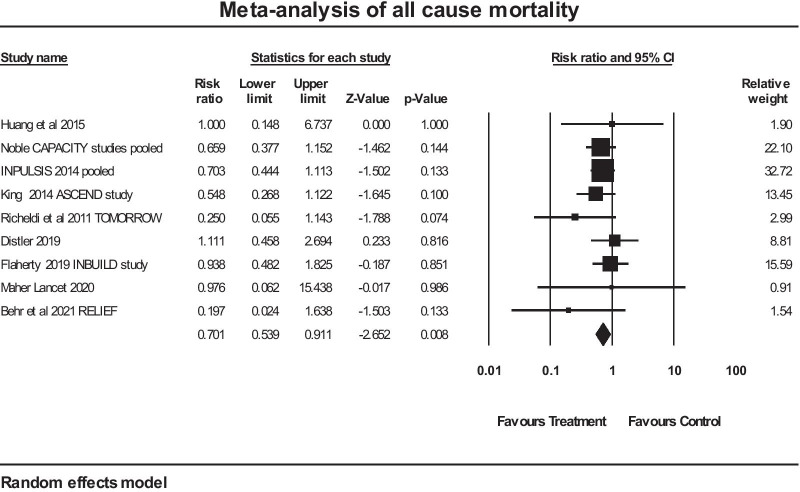
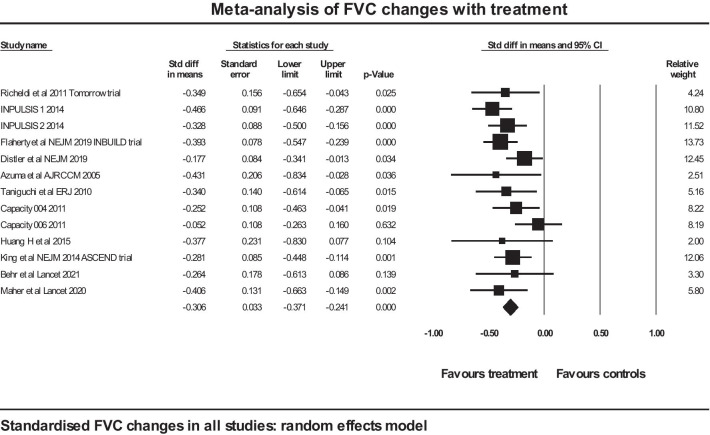
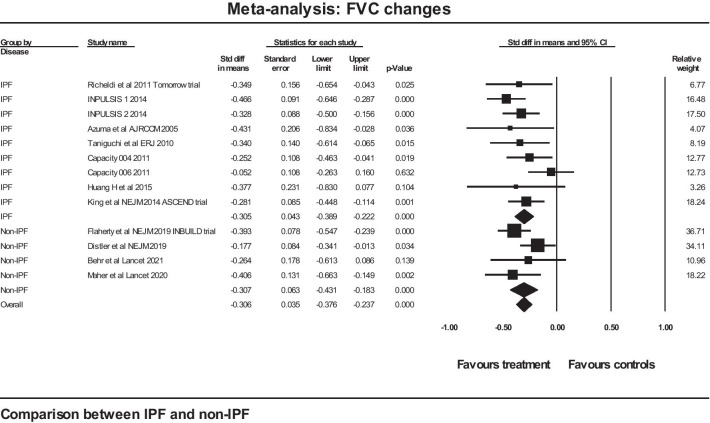
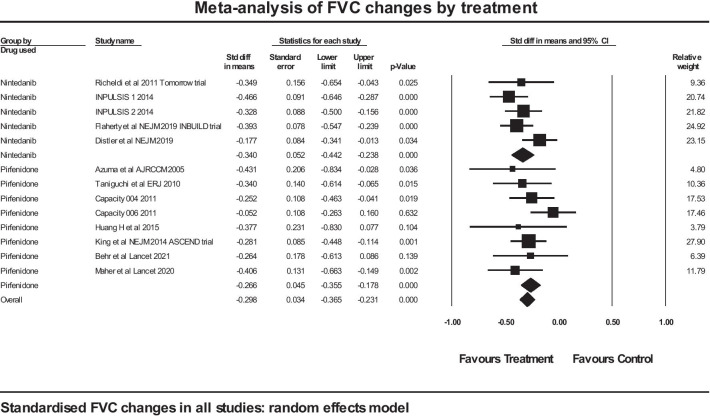
13 trials of antifibrotic therapy were pooled in a meta-analysis (with pirfenidone and nintedanib considered together as anti-fibrotic therapy). The change in FVC was expressed as a standardised difference to allow pooling of percentage and absolute changes. The mean effect size in the IPF studies was - 0.305 (SE 0.043) (p < 0.001) and in the non-IPF studies the figures were - 0.307 (SE 0.063) (p < 0.001). There was no evidence of any difference between the two groups for standardised rate of FVC decline (p = 0.979). Pooling IPF and non-IPF showed a significant reduction in mortality, with mean risk ratio of 07.01 in favour of antifibrotic therapy (p = 0.008). A separate analysis restricted to non-IPF did not show a significant reduction in mortality (risk ratio 0.908 (0.547 to 1.508), p = 0.71.
Anti-fibrotic therapy offers protection against the rate of decline in FVC in progressive lung fibrosis, with similar efficacy shown between the two anti-fibrotic agents currently in clinical use. There was no significant difference in efficacy of antifibrotic therapy whether the underlying condition was IPF or non-IPF with progressive fibrosis, supporting the hypothesis of a common pathogenesis. The data in this analysis was insufficient to be confident about a reduction in mortality in non-IPF with anti-fibrotic therapy. Trial Registration PROSPERO, registration number CRD42021266046.
研究问题
比较尼达尼布和吡非尼酮治疗进行性肺纤维化的疗效;比较抗纤维化治疗(将尼达尼布和吡非尼酮归为一组)在特发性肺纤维化患者与未分类为特发性肺纤维化的进行性肺纤维化患者中的疗效。
对包括 MEDLINE、EMBASE、PubMed 和 clinicaltrials.gov 在内的数据库进行了检索。如果研究是随机对照试验,比较尼达尼布或吡非尼酮在特发性肺纤维化或非特发性肺纤维化患者中的疗效,且可提取死亡率或用力肺活量(FVC)下降的数据,则将其纳入研究。对所选研究中 FVC 的变化进行了随机效应荟萃分析,并在可能的情况下对死亡率进行了分析。
抗纤维化治疗的 13 项试验进行了荟萃分析(将吡非尼酮和尼达尼布一起视为抗纤维化治疗)。FVC 的变化表示为标准化差异,以允许汇总百分比和绝对变化。特发性肺纤维化研究的平均效应大小为-0.305(SE 0.043)(p<0.001),而非特发性肺纤维化研究的数值为-0.307(SE 0.063)(p<0.001)。两组间 FVC 下降的标准化率无差异(p=0.979)。汇总特发性肺纤维化和非特发性肺纤维化显示死亡率显著降低,抗纤维化治疗的平均风险比为 07.01(p=0.008)。单独对非特发性肺纤维化的分析显示死亡率无显著降低(风险比 0.908(0.547 至 1.508),p=0.71)。
抗纤维化治疗可防止进行性肺纤维化患者的 FVC 下降速度,两种目前临床使用的抗纤维化药物的疗效相似。无论潜在疾病是特发性肺纤维化还是非特发性肺纤维化伴有进行性纤维化,抗纤维化治疗的疗效均无显著差异,支持共同发病机制的假说。本分析中的数据不足以确定非特发性肺纤维化患者使用抗纤维化治疗是否能降低死亡率。
PROSPERO,注册号 CRD42021266046。