Lee Wei-Chieh, Lee Pai-Wei, Wu Po-Jui, Fang Yen-Nan, Chen Huang-Chung, Lin Yu-Sheng, Fang Hsiu-Yu, Chang Shang-Hung, Liu Ping-Yen, Chen Mien-Cheng
Institute of Clinical Medicine, College of Medicine, National Cheng Kung University, Tainan, Taiwan.
Division of Cardiology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, 123 Ta Pei Road, Niao Sung District, Kaohsiung City, 83301, Taiwan.
Thromb J. 2021 Dec 11;19(1):98. doi: 10.1186/s12959-021-00351-1.
Long-term oral anticoagulant should be considered or recommended in patients with atrial fibrillation (AF) and CHA2DS2VASc score ≥ 1 for stroke prevention. Warfarin and different direct oral anticoagulants (DOACs) are metabolized differently by the kidney. The impact on renal function after long-term use of anticoagulants in the patients with AF remains unclear. This study aimed to compare DOACs and warfarin's impact on the decline in renal function from a large cohort with AF.
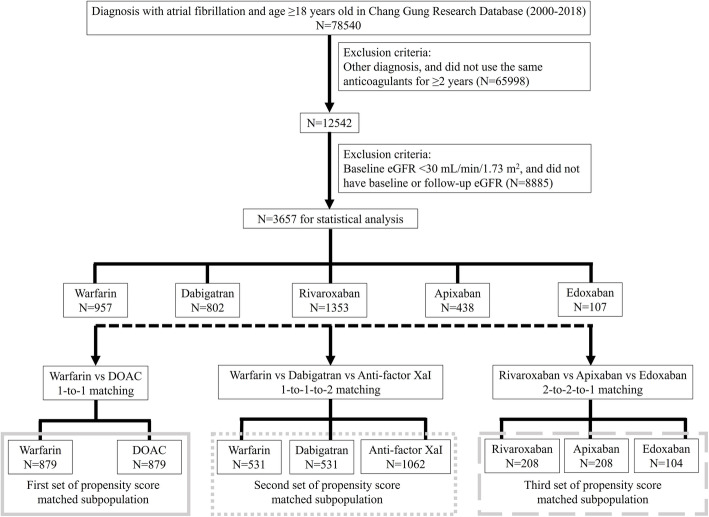
This study included patients with nonvalvular AF from 2000 to 2018, mainly through the medical history (ICD code) of the Chang Gung Research Database. Baseline estimated glomerular filtration rate (eGFR), follow-up eGFR and the change in eGFR between 2-year eGFR and baseline eGFR were compared between different DOACs and warfarin after propensity score matching. The primary study endpoint was acute kidney injury (AKI).
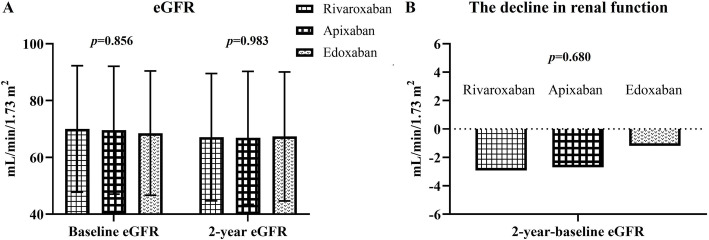
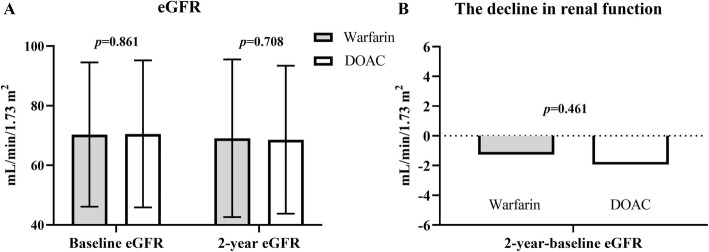
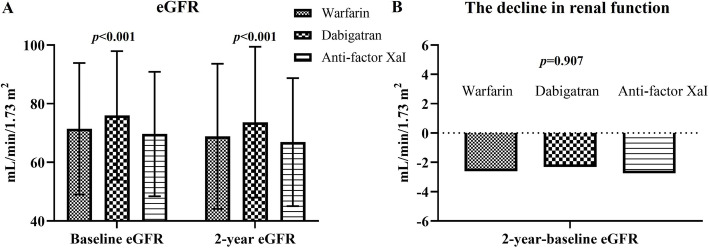
3657 patients were enrolled in this study and the mean observation time was 3.3 ± 0.9 years. During the observation period, there was a significantly higher incidence of AKI during follow-up in the warfarin group than in the different DOAC groups before and after propensity score matching (before: warfarin vs. DOAC: 9.2% vs. 5.2%, p < 0.001; after: warfarin vs. DOAC: 8.9% vs. 4.4%, p < 0.001). There was no difference in the incidence of AKI between dabigatran group and anti-factor Xa inhibitor group after propensity score matching. The incidence of AKI was similar among rivaroxaban, apixaban and edoxaban groups after propensity score matching. The change in eGFR between 2-year eGFR and baseline eGFR did not differ between the warfarin and DOAC groups after propensity score matching (warfarin vs. DOAC: - 1.27 ± 20.32 vs. -1.94 ± 17.24 mL/min/1.73 m, p = 0.461).
During the mean observation time of 3.3 ± 0.9 years, warfarin was associated with a higher incidence of AKI compared with DOACs. The decline in renal function did not differ among warfarin and different DOAC groups.
对于心房颤动(AF)且CHA2DS2VASc评分≥1的患者,应考虑或推荐长期口服抗凝药以预防卒中。华法林和不同的直接口服抗凝药(DOACs)在肾脏中的代谢方式不同。长期使用抗凝药对AF患者肾功能的影响仍不清楚。本研究旨在比较DOACs和华法林对一大群AF患者肾功能下降的影响。
本研究纳入了2000年至2018年的非瓣膜性AF患者,主要通过长庚研究数据库的病史(ICD编码)进行。在倾向得分匹配后,比较不同DOACs和华法林之间的基线估计肾小球滤过率(eGFR)、随访eGFR以及2年eGFR与基线eGFR之间eGFR的变化。主要研究终点是急性肾损伤(AKI)。
本研究共纳入3657例患者,平均观察时间为3.3±0.9年。在观察期内,倾向得分匹配前后,华法林组随访期间AKI的发生率显著高于不同DOAC组(匹配前:华法林组与DOAC组:9.2%对5.2%,p<0.001;匹配后:华法林组与DOAC组:8.9%对4.4%,p<0.001)。倾向得分匹配后,达比加群组和抗Xa因子抑制剂组之间AKI的发生率没有差异。倾向得分匹配后,利伐沙班、阿哌沙班和依度沙班组之间AKI的发生率相似。倾向得分匹配后,华法林组和DOAC组之间2年eGFR与基线eGFR之间eGFR的变化没有差异(华法林组与DOAC组:-1.27±20.32对-1.94±17.24 mL/min/1.73 m²,p = 0.461)。
在平均观察时间3.3±0.9年期间,与DOACs相比,华法林与更高的AKI发生率相关。华法林组和不同DOAC组之间肾功能的下降没有差异。