Department of Paediatric Oncology, Justus-Liebig- University Giessen, Giessen, Germany; Medical Faculty, Martin Luther University Halle-Wittenberg, Halle, Germany.
Department of Paediatric Haematology-Oncology, Sorbonne Université and APHP-SIRIC CURAMUS Hôpital a Trousseau, Paris, France.
Lancet Oncol. 2022 Jan;23(1):125-137. doi: 10.1016/S1470-2045(21)00470-8. Epub 2021 Dec 9.
Children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma achieve an event-free survival at 5 years of about 90% after treatment with vincristine, etoposide, prednisone, and doxorubicin (OEPA) followed by cyclophosphamide, vincristine, prednisone, and procarbazine (COPP) and radiotherapy, but long-term treatment effects affect survival and quality of life. We aimed to investigate whether radiotherapy can be omitted in patients with morphological and metabolic adequate response to OEPA and whether modified consolidation chemotherapy reduces gonadotoxicity.
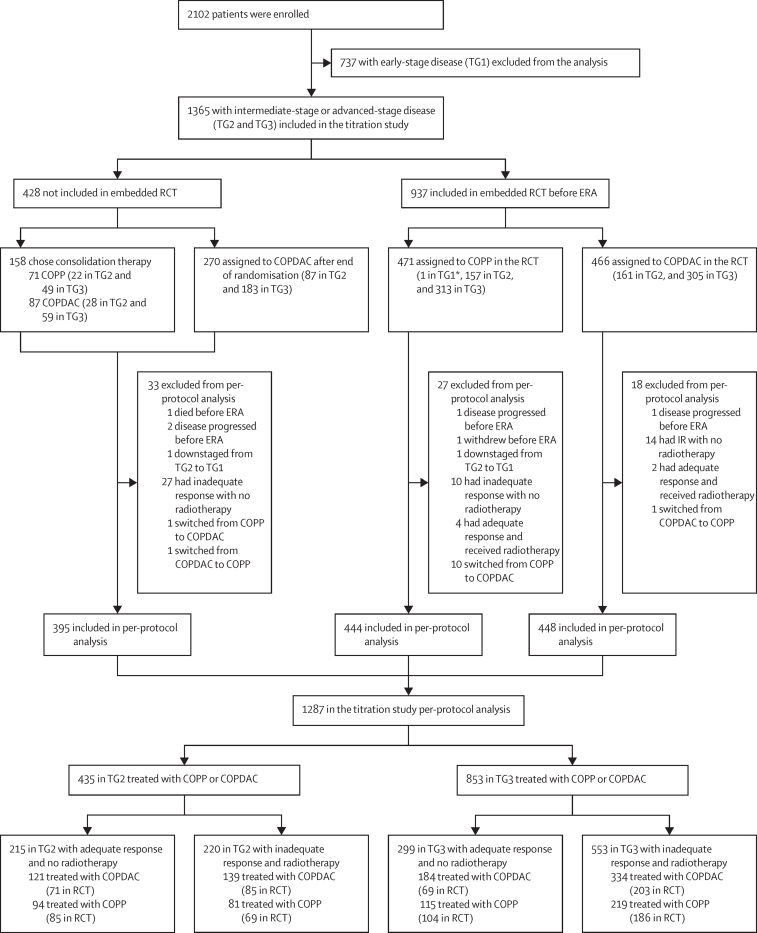
Our study was designed as a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial, and was carried out at 186 hospital sites across 16 European countries. Children and adolescents with newly diagnosed intermediate-stage (treatment group 2) and advanced-stage (treatment group 3) classical Hodgkin lymphoma who were younger than 18 years and stratified according to risk using Ann Arbor disease stages IIAE, IIB, IIBE, IIIA, IIIAE, IIIB, IIIBE, and all stages IV (A, B, AE, and BE) were included in the study. Patients with early disease (treatment group 1) were excluded from this analysis. All patients were treated with two cycles of OEPA (1·5 mg/m vincristine taken intravenously capped at 2 mg, on days 1, 8, and 15; 125 mg/m etoposide taken intravenously on days 1-5; 60 mg/m prednisone taken orally on days 1-15; and 40 mg/m doxorubicin taken intravenously on days 1 and 15). Patients were randomly assigned to two (treatment group 2) or four (treatment group 3) cycles of COPP (500 mg/m cyclophosphamide taken intravenously on days 1 and 8; 1·5 mg/m vincristine taken intravenously capped at 2 mg, on days 1 and 8; 40 mg/m prednisone taken orally on days 1 to 15; and 100 mg/m procarbazine taken orally on days 1 to 15) or COPDAC, which was identical to COPP except that 250 mg/m dacarbazine administered intravenously on days 1 to 3 replaced procarbazine. The method of randomisation (1:1) was minimisation with stochastic component and was centrally stratified by treatment group, country, trial sites, and sex. The primary endpoint was event-free survival, defined as time from treatment start until the first of the following events: death from any cause, progression or relapse of classical Hodgkin lymphoma, or occurrence of secondary malignancy. The primary objectives were maintaining 90% event-free survival at 5 years in patients with adequate response to OEPA treated without radiotherapy and to exclude a decrease of 8% in event-free survival at 5 years in the embedded COPDAC versus COPP randomisation to show non-inferiority of COPDAC. Efficacy analyses are reported per protocol and safety in the intention-to-treat population. The trial is registered with ClinicalTrials.gov (trial number NCT00433459) and EUDRACT (trial number 2006-000995-33), and is closed to recruitment.
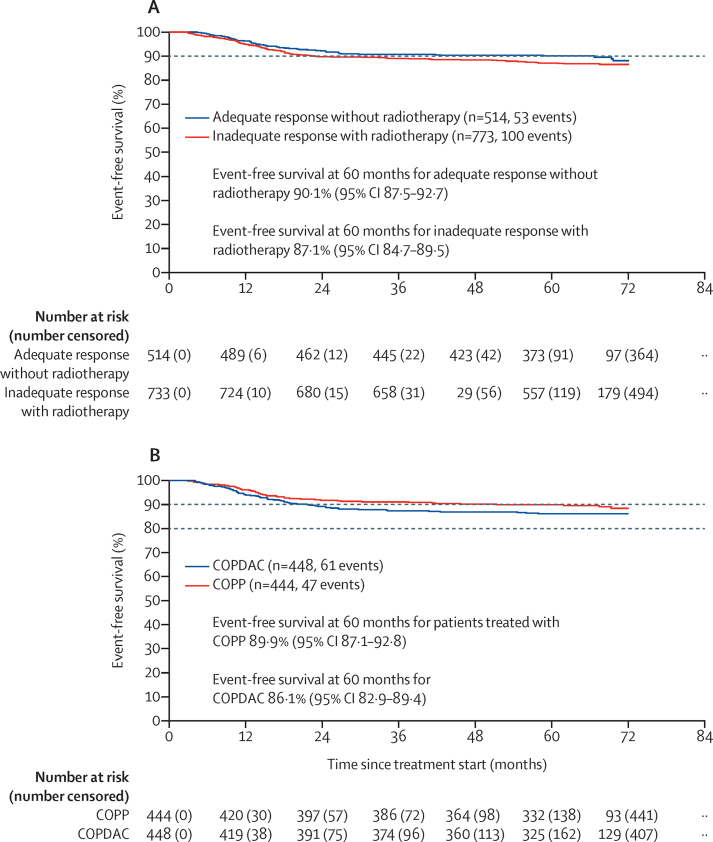
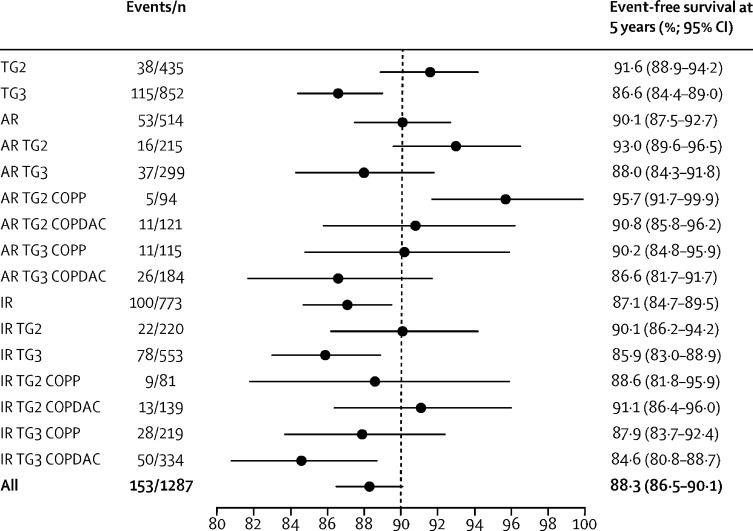
Between Jan 31, 2007, and Jan 30, 2013, 2102 patients were recruited. 737 (35%) of the 2102 recruited patients were in treatment group 1 (early-stage disease) and were not included in our analysis. 1365 (65%) of the 2102 patients were in treatment group 2 (intermediate-stage disease; n=455) and treatment group 3 (advanced-stage disease; n=910). Of these 1365, 1287 (94%) patients (435 [34%] of 1287 in treatment group 2 and 852 [66%] of 1287 in treatment group 3) were included in the titration trial per-protocol analysis. 937 (69%) of 1365 patients were randomly assigned to COPP (n=471) or COPDAC (n=466) in the embedded trial. Median follow-up was 66·5 months (IQR 62·7-71·7). Of 1287 patients in the per-protocol group, 514 (40%) had an adequate response to treatment and were not treated with radiotherapy (215 [49%] of 435 in treatment group 2 and 299 [35%] of 852 in treatment group 3). 773 (60%) of 1287 patients with inadequate response were scheduled for radiotherapy (220 [51%] of 435 in the treatment group 2 and 553 [65%] of 852 in treatment group 3. In patients who responded adequately, event-free survival rates at 5 years were 90·1% (95% CI 87·5-92·7). event-free survival rates at 5 years in 892 patients who were randomly assigned to treatment and analysed per protocol were 89·9% (95% CI 87·1-92·8) for COPP (n=444) versus 86·1% (82·9-89·4) for COPDAC (n=448). The COPDAC minus COPP difference in event-free survival at 5 years was -3·7% (-8·0 to 0·6). The most common grade 3-4 adverse events (intention-to-treat population) were decreased haemoglobin (205 [15%] of 1365 patients during OEPA vs 37 [7%] of 528 treated with COPP vs 20 [2%] of 819 treated with COPDAC), decreased white blood cells (815 [60%] vs 231 [44%] vs 84 [10%]), and decreased neutrophils (1160 [85%] vs 223 [42%] vs 174 [21%]). One patient in treatment group 2 died of sepsis after the first cycle of OEPA; no other treatment-related deaths occurred.
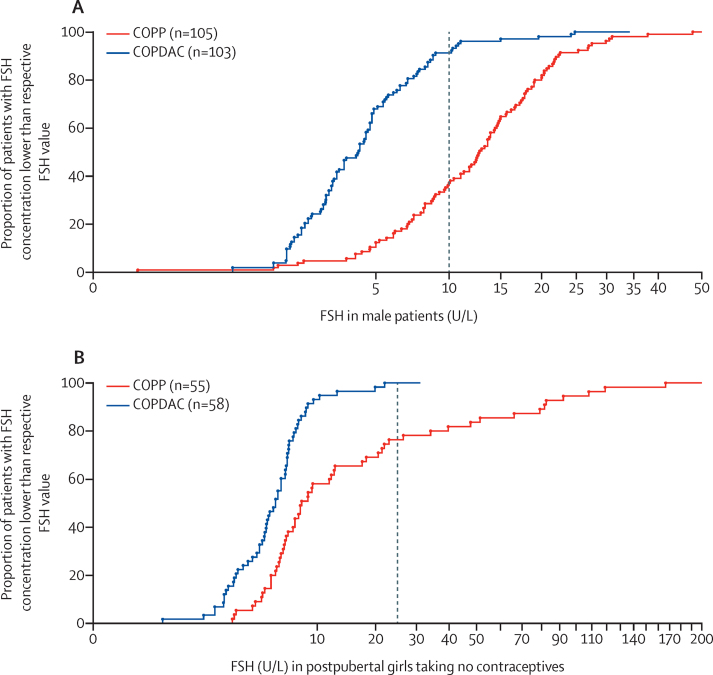
Our results show that radiotherapy can be omitted in patients who adequately respond to treatment, when consolidated with COPP or COPDAC. COPDAC might be less effective, but is substantially less gonadotoxic than COPP. A high proportion of patients could therefore be spared radiotherapy, eventually reducing the late effects of treatment. With more refined criteria for response assessment, the number of patients who receive radiotherapy will be further decreased.
Deutsche Krebshilfe, Elternverein für Krebs-und leukämiekranke Kinder Gießen, Kinderkrebsstiftung Mainz, Tour der Hoffnung, Menschen für Kinder, Programme Hospitalier de Recherche Clinique, and Cancer Research UK.
接受长春新碱、依托泊苷、泼尼松和多柔比星(OEPA)联合环磷酰胺、长春新碱、泼尼松和丙卡巴肼(COPP)和放疗的中期和晚期经典霍奇金淋巴瘤患儿和青少年,5 年无事件生存率约为 90%,但长期治疗效果会影响生存和生活质量。我们旨在研究对 OEPA 有形态学和代谢充分反应的患者能否省略放疗,以及改良巩固化疗是否会降低性腺毒性。
我们的研究是一项滴定研究,采用开放标签、嵌入式、多国、非劣效性、随机对照试验设计,并在 16 个欧洲国家的 186 家医院进行。新诊断为中期(治疗组 2)和晚期(治疗组 3)经典霍奇金淋巴瘤的年龄小于 18 岁且根据安阿伯疾病分期 IIAE、IIB、IIBE、III A、III AE、III B、III BE 和所有 IV 期(A、B、AE 和 BE)分层的儿童和青少年被纳入研究。早期疾病(治疗组 1)的患者被排除在本分析之外。所有患者均接受两个周期的 OEPA(1.5mg/m 长春新碱静脉注射,最大剂量为 2mg,第 1、8 和 15 天;125mg/m 依托泊苷静脉注射,第 1-5 天;60mg/m 泼尼松口服,第 1-15 天;40mg/m 多柔比星静脉注射,第 1 和 15 天)治疗。患者随机分配至两组(治疗组 2)或四组(治疗组 3)接受 COPP(500mg/m 环磷酰胺静脉注射,第 1 和 8 天;1.5mg/m 长春新碱静脉注射,最大剂量为 2mg,第 1 和 8 天;40mg/m 泼尼松口服,第 1-15 天;100mg/m 丙卡巴肼口服,第 1-15 天)或 COPDAC,后者与 COPP 相同,只是用 250mg/m 达卡巴嗪静脉注射代替丙卡巴肼,第 1-3 天。随机化方法(1:1)是最小化与随机成分相结合,并通过治疗组、国家、试验地点和性别进行中心分层。主要终点是无事件生存,定义为从治疗开始到以下任何事件发生的时间:任何原因导致的死亡、经典霍奇金淋巴瘤的进展或复发、或继发性恶性肿瘤的发生。主要目的是在对 OEPA 有充分反应的患者中维持 5 年 90%的无事件生存率,而无需放疗,并排除嵌入的 COPDAC 与 COPP 随机化时 5 年无事件生存率下降 8%,以证明 COPDAC 的非劣效性。疗效分析按方案进行,安全性分析采用意向治疗人群。该试验在 ClinicalTrials.gov(试验编号:NCT00433459)和 EUDRACT(试验编号:2006-000995-33)注册,并已关闭入组。
2007 年 1 月 31 日至 2013 年 1 月 30 日期间,共招募了 2102 名患者。2102 名招募的患者中有 737 名(35%)处于早期疾病(治疗组 1),未纳入本分析。2102 名患者中有 1365 名(65%)处于中期疾病(治疗组 2;n=455)和晚期疾病(治疗组 3;n=910)。其中 1287 名患者(94%)(治疗组 2 中有 435 名[34%],治疗组 3 中有 852 名[66%])按方案进行了滴定试验分析。1365 名患者中有 1287 名(937 名)(937 名)随机分配至 COPP(n=471)或 COPDAC(n=466)在嵌入式试验中。中位随访时间为 66.5 个月(IQR 62.7-71.7)。在按方案分组的 1287 名患者中,514 名(40%)对治疗有充分反应,无需放疗(治疗组 2 中有 215 名[49%],治疗组 3 中有 299 名[35%])。对治疗反应不足的 773 名患者(60%)计划进行放疗(治疗组 2 中有 220 名[51%],治疗组 3 中有 553 名[65%])。在对治疗有充分反应的患者中,5 年无事件生存率为 90.1%(95%CI 87.5-92.7)。在按方案随机分配并分析的 892 名患者中,COPP(n=444)的 5 年无事件生存率为 89.9%(95%CI 87.1-92.8),COPDAC(n=448)为 86.1%(82.9-89.4)。COPDAC 与 COPP 相比,5 年无事件生存率的差异为-3.7%(-8.0 至 0.6)。最常见的 3-4 级不良事件(意向治疗人群)是血红蛋白减少(1365 名患者中有 205 名[15%]在 OEPA 期间,528 名接受 COPP 治疗的患者中有 37 名[7%],819 名接受 COPDAC 治疗的患者中有 20 名[2%])、白细胞减少(815 名[60%]与 231 名[44%]与 84 名[10%])和中性粒细胞减少(1160 名[85%]与 223 名[42%]与 174 名[21%])。治疗组 2 中有 1 名患者在接受 OEPA 第一周期后死于败血症;没有其他与治疗相关的死亡。
我们的结果表明,对治疗有充分反应的患者可以省略放疗,当与 COPP 或 COPDAC 联合巩固时。COPDAC 可能效果较差,但性腺毒性明显低于 COPP。因此,很大一部分患者可以避免放疗,最终减少治疗的晚期影响。随着对反应评估标准的进一步细化,接受放疗的患者数量将进一步减少。
德国癌症援助、癌症和白血病儿童父母协会吉森、美因茨慈善基金会、盖尔森基兴希望之旅、儿童与青少年癌症基金会、医院临床研究计划和英国癌症研究中心。