Pediatric Oncology, Cancer Center Amsterdam, Emma Children's Hospital, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Department of Paediatric Haemato-Oncology, Princess Máxima Center for Pediatric Oncology, Utrecht, The Netherlands.
Hum Reprod. 2024 Nov 1;39(11):2411-2422. doi: 10.1093/humrep/deae204.
What is the impact of the EuroNet-PHL-C2 treatment for boys with classical Hodgkin lymphoma (cHL) on semen parameters?
More than half of the patients (52%, n = 16/31) had oligozoospermia or azoospermia at 2 years from cHL diagnosis; particularly boys treated for advanced-stage cHL had low sperm counts and motility.
Chemotherapy and radiotherapy to the inguinal region or testes can impair spermatogenesis and result in reduced fertility. The EuroNet-PHL-C2 trial aims to minimize radiotherapy in standard childhood cHL treatment, by intensifying chemotherapy. The present study aims to assess the (gonadotoxic) impact of this treatment protocol on semen parameters and reproductive hormones in boys aged ≤18 years.
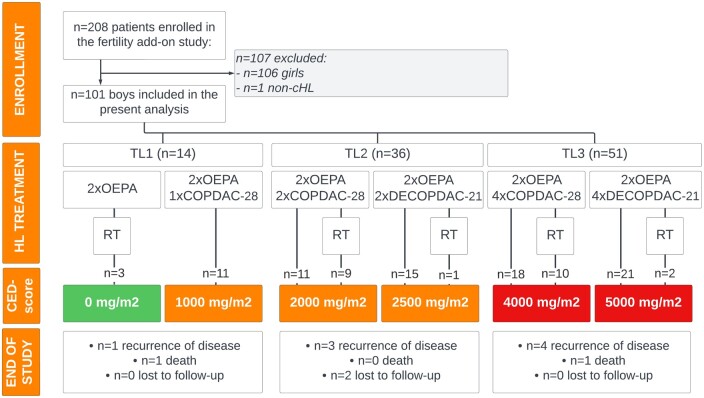
STUDY DESIGN, SIZE, DURATION: This international, prospective, multi-centre cohort study was an add-on study to the randomized phase-3 EuroNet-PHL-C2 trial, where the efficacy of standard cHL treatment with OEPA-COPDAC-28 (OEPA: vincristine, etoposide, prednisone, and doxorubicin; COPDAC-28: cyclophosphamide, vincristine, prednisone, and dacarbazine) was compared to intensified OEPA-DECOPDAC-21 chemotherapy (DECOPDAC-21: COPDAC with additional doxorubicin and etoposide and 25% more cyclophosphamide). Patients were recruited between January 2017 and September 2021.
PARTICIPANTS/MATERIALS, SETTING, METHODS: Eligibility criteria included male patients, diagnosed with classical HL before or at the age of 18 years, and treated according to the EuroNet-PHL-C2 protocol in any of the 18 participating sites in the Netherlands, Germany, Belgium, Czech Republic, and Austria. Sperm parameters (sperm concentration, progressive motility, sperm volume, and calculated total motile sperm count) were assessed at diagnosis and 2 years after diagnosis in (post)pubertal boys. Laboratory measurements (serum follicle-stimulating hormone (FSH) and inhibin B) were performed in samples drawn at diagnosis, during treatment (2-3 times), and at 2 years post-diagnosis, and (age-adjusted) analyses were conducted separately for pre-pubertal and (post)pubertal boys. Outcomes were compared between the treatment levels (TL1, TL2, and TL3) and consolidation treatment schemes (COPDAC-28 and DECOPDAC-21).
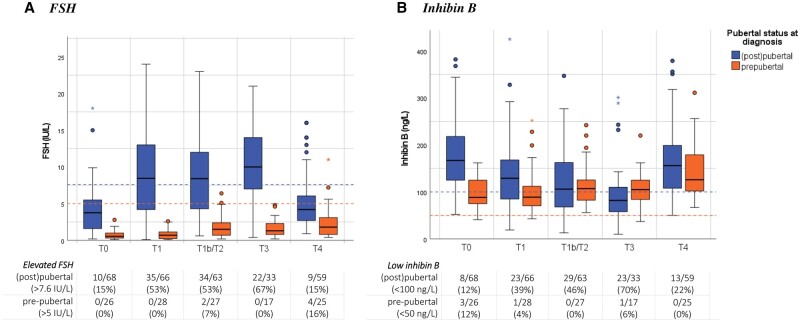
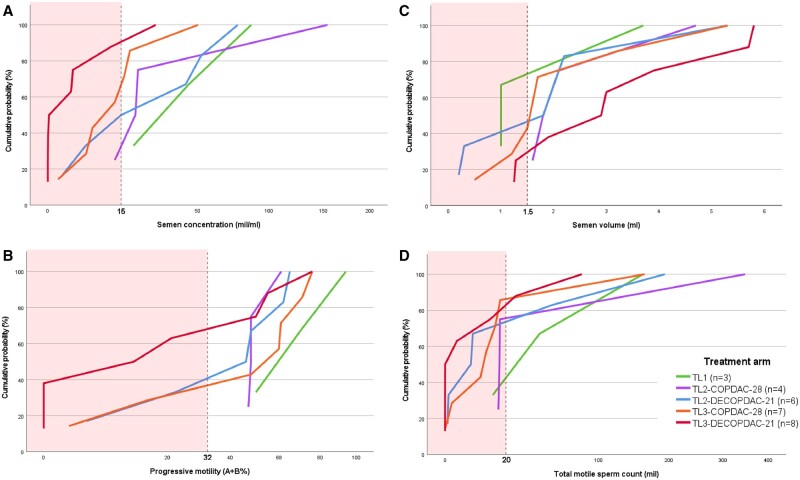
In total, 101 boys were included in the present analysis: 73 were (post)pubertal (median age 15.4 years, (IQR 14.4; 16.6), 10 TL1, 29 TL2, 34 TL3, 62% of TL2/3 patients received COPDAC-28) and 28 boys were pre-pubertal (median age 9.6 years (IQR 6.6; 11.4), 4 TL1, 7 TL2, 17 TL3, 38% of TL2/3 patients received COPDAC-28). The study included six boys who had received pelvic radiotherapy; none were irradiated in the inguinal or testicular area. At diagnosis, 48 (post)pubertal boys delivered semen for cryopreservation; 19 (40%) semen samples were oligospermic and 4 (8%) were azoospermic. Low sperm concentration (<15 mil/ml) appeared to be related to the HL disease itself, with a higher prevalence in boys who presented with B symptoms (76% vs 26%, aOR 2.3 (95% CI 1.0; 3.8), P = 0.001) compared to those without such symptoms. At 2 -years post-diagnosis, 31 boys provided semen samples for analysis, of whom 12 (39%) boys had oligozoospermia and 4 (13%) had azoospermia, while 22 boys (71%) had low total motile sperm counts (TMSC) (<20 mil). Specifically, the eight boys in the TL3 group treated with DECOPDAC-21 consolidation had low sperm counts and low progressive motility after 2 years (i.e. median sperm count 1.4 mil/ml (IQR <0.1; 5.3), n = 7 (88%), low sperm concentration, low median progressive motility 16.5% (IQR 0.0; 51.2), respectively). Age-adjusted serum FSH levels were significantly raised and inhibin B levels (and inhibin B:FSH ratios) were decreased during chemotherapy in (post)pubertal boys, with subsequent normalization in 80% (for FSH) and 60% (for inhibin B) of boys after 2 years. Only 4 out of the 14 (post)pubertal boys (29%) with low sperm concentrations after 2 years had elevated FSH (>7.6 IU/l), while 7 (50%) had low inhibin B levels (<100 ng/l). In pre-pubertal boys, reproductive hormones were low overall and remained relatively stable during chemotherapy.
LIMITATIONS, REASONS FOR CAUTION: The present analyses included sperm and laboratory measurements up to 2 years post-diagnosis. Long-term reproductive outcomes and potential recovery of spermatogenesis remain unknown, while recovery was reported up to 5- or even 10-year post-chemotherapy in previous studies.Boys who were pre-pubertal at diagnosis were still too young and/or physically not able to deliver semen after 2 years and we could not assess a potential difference in gonadotoxicity according to pubertal state at the time of treatment. Overall, the statistical power of the analyses on sperm concentration and quality after 2 years was limited.
Results of the semen analyses conducted among the 31 boys who had provided a semen sample at 2 years post-treatment were generally poor. However, additional long-term and adequately powered data are crucial to assess the potential recovery and clinical impact on fertility. The participating boys will be invited to deliver a semen sample after 5 years. Until these data become available, benefits of intensified chemotherapy in cHL treatment to reduce radiotherapy and lower risk for development of secondary tumours should be carefully weighed against potentially increased risk of other late effects, such as diminished fertility due to the increased chemotherapy burden. Boys with newly diagnosed cHL should be encouraged to deliver sperm for cryopreservation whenever possible. However, patients and clinicians should also realize that the overall state of disease and inflammatory milieu of cHL can negatively affect sperm quality and thereby reduce chance of successful fertility preservation. Furthermore, the measurement of FSH and inhibin B appears to be of low value in predicting low sperm quality at two years from cHL treatment.
STUDY FUNDING/COMPETING INTEREST(S): This study was funded by the Dutch charity foundation KiKa (project 257) that funds research on all forms of childhood cancer. C.M.-K., D.K., W.H.W., D.H., MC, A.U., and A.B. were involved in the development of the EuroNet-PHL-C2 regimen. The other authors declare no potential conflict of interest.
N/A.
EuroNet-PHL-C2 治疗方案对经典霍奇金淋巴瘤(cHL)男孩的精液参数有何影响?
超过一半的患者(52%,n=31/60)在 cHL 诊断后 2 年时出现少精子症或无精子症;特别是接受晚期 cHL 治疗的男孩精子计数和活力较低。
对腹股沟区或睾丸进行化疗和放疗会损害生精功能,导致生育能力下降。EuroNet-PHL-C2 试验旨在通过强化化疗来最大限度地减少标准儿童 cHL 治疗中的放疗,本研究旨在评估该治疗方案对≤18 岁男孩精液参数和生殖激素的(性腺毒性)影响。
研究设计、大小、持续时间:这是一项国际性、前瞻性、多中心队列研究,是随机 3 期 EuroNet-PHL-C2 试验的附加研究,比较了 OEPA-COPDAC-28(OEPA:长春新碱、依托泊苷、泼尼松和多柔比星;COPDAC-28:环磷酰胺、长春新碱、泼尼松和达卡巴嗪)标准 cHL 治疗与强化 OEPA-DECOPDAC-21 化疗(DECOPDAC-21:COPDAC 加多柔比星和依托泊苷,环磷酰胺增加 25%)的疗效。患者于 2017 年 1 月至 2021 年 9 月期间招募。
参与者/材料、设置、方法:符合条件的患者包括男性,在 18 岁之前或 18 岁时被诊断为经典 HL,根据 EuroNet-PHL-C2 方案在荷兰、德国、比利时、捷克共和国和奥地利的 18 个参与地点之一接受治疗。在青春期后男孩中,在诊断时和诊断后 2 年时评估精子参数(精子浓度、前向运动精子比例、精子体积和计算的总活动精子数)。在诊断时、治疗期间(2-3 次)和诊断后 2 年时采集实验室测量(血清卵泡刺激素(FSH)和抑制素 B)样本,并分别对青春期前和(青春期后)男孩进行年龄调整分析。将治疗水平(TL1、TL2 和 TL3)和巩固治疗方案(COPDAC-28 和 DECOPDAC-21)之间的结果进行比较。
本分析共纳入 101 名男孩:73 名(青春期后)(中位年龄 15.4 岁,[IQR 14.4;16.6],10 名 TL1,29 名 TL2,34 名 TL3,62%的 TL2/3 患者接受 COPDAC-28)和 28 名青春期前男孩(中位年龄 9.6 岁,[IQR 6.6;11.4],4 名 TL1,7 名 TL2,17 名 TL3,38%的 TL2/3 患者接受 COPDAC-28)。研究纳入了 6 名接受盆腔放疗的男孩;均未对腹股沟或睾丸区域进行放疗。在诊断时,48 名(青春期后)男孩提供精液进行冷冻保存;19 名(40%)精液样本为少精子症,4 名(8%)为无精子症。低精子浓度(<15 mil/ml)似乎与 HL 疾病本身有关,与无 B 症状的男孩相比,有 B 症状的男孩的患病率更高(76%比 26%,优势比 2.3(95%CI 1.0;3.8),P=0.001)。在诊断后 2 年时,31 名男孩提供精液样本进行分析,其中 12 名(39%)男孩出现少精子症,4 名(13%)出现无精子症,而 22 名(71%)男孩的总活动精子数(TMSC)较低(<20 mil)。具体来说,接受 DECOPDAC-21 巩固治疗的 TL3 组的 8 名男孩在 2 年后精子计数低且前向运动精子比例低(即中位数精子计数 1.4 mil/ml(IQR <0.1;5.3),n=7(88%),低精子浓度,中位数前向运动精子比例低 16.5%(IQR 0.0;51.2))。在(青春期后)男孩中,化疗期间血清 FSH 水平显著升高,抑制素 B 水平(和抑制素 B:FSH 比值)降低,80%(FSH)和 60%(抑制素 B)的男孩在 2 年后恢复正常。在 2 年后精子浓度低的 14 名(青春期后)男孩中,只有 4 名(29%)的 FSH 升高(>7.6 IU/l),而 7 名(50%)的抑制素 B 水平低(<100 ng/l)。在青春期前男孩中,生殖激素总体较低,在化疗期间相对稳定。
局限性、谨慎的原因:本分析包括诊断后 2 年内的精子和实验室测量。长期生殖结果和潜在的精子发生恢复情况仍不清楚,而以前的研究报告称,在化疗后 5 年或甚至 10 年内恢复了生育能力。诊断时处于青春期前的男孩年龄太小或身体上无法在 2 年后提供精液,我们无法根据治疗时的青春期状态评估性腺毒性的差异。总体而言,2 年后精子浓度和质量分析的统计功效有限。
在接受 2 年治疗后提供精液样本的 31 名男孩中,精液分析的结果普遍较差。然而,需要更多的长期和充分的有力数据来评估潜在的恢复和对生育的潜在临床影响。参与的男孩将被邀请在 5 年后提供精液样本。在这些数据可用之前,为了降低放疗风险和降低发展继发性肿瘤的风险,应谨慎权衡在 cHL 治疗中强化化疗以减少放疗和增加化疗负担的潜在益处。应鼓励新诊断的 cHL 男孩尽可能多地提供精液进行冷冻保存。然而,患者和临床医生也应该意识到,cHL 的疾病状态和炎症环境会对精子质量产生负面影响,从而降低成功生育保护的机会。此外,测量 FSH 和抑制素 B 似乎对预测 cHL 治疗 2 年后的精子质量价值有限。
研究资助/利益冲突:本研究由荷兰慈善基金会 KiKa(项目 257)资助,该基金会资助所有形式的儿童癌症研究。C.M.-K.、D.K.、W.H.W.、D.H.、MC、A.U.和 A.B.参与了 EuroNet-PHL-C2 方案的制定。其他作者声明不存在潜在的利益冲突。
无。